- Record: found
- Abstract: found
- Article: found
Tocilizumab and remdesivir in hospitalized patients with severe COVID-19 pneumonia: a randomized clinical trial
Read this article at
Abstract
Purpose
Trials of tocilizumab in patients with severe COVID-19 pneumonia have demonstrated mixed results, and the role of tocilizumab in combination with other treatments is uncertain. Here we evaluated whether tocilizumab plus remdesivir provides greater benefit than remdesivir alone in patients with severe COVID-19 pneumonia.
Methods
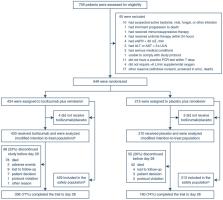
This randomized, double-blind, placebo-controlled, multicenter trial included patients hospitalized with severe COVID-19 pneumonia requiring > 6 L/min supplemental oxygen. Patients were randomly assigned (2:1 ratio) to receive tocilizumab 8 mg/kg or placebo intravenously plus ≤ 10 days of remdesivir. The primary outcome was time from randomization to hospital discharge or “ready for discharge” (defined as category 1, assessed by the investigator on a 7-category ordinal scale of clinical status) to day 28. Patients were followed for 60 days.
Results
Among 649 enrolled patients, 434 were randomly assigned to tocilizumab plus remdesivir and 215 to placebo plus remdesivir. 566 patients (88.2%) received corticosteroids during the trial to day 28. Median time from randomization to hospital discharge or “ready for discharge” was 14 (95% CI 12–15) days with tocilizumab plus remdesivir and 14 (95% CI 11–16) days with placebo plus remdesivir [log-rank P = 0.74; Cox proportional hazards ratio 0.97 (95% CI 0.78–1.19)]. Serious adverse events occurred in 128 (29.8%) tocilizumab plus remdesivir and 72 (33.8%) placebo plus remdesivir patients; 78 (18.2%) and 42 (19.7%) patients, respectively, died by day 28.
Related collections
Most cited references17
- Record: found
- Abstract: found
- Article: found
Remdesivir for the Treatment of Covid-19 — Final Report
- Record: found
- Abstract: found
- Article: not found
Repurposed Antiviral Drugs for Covid-19 — Interim WHO Solidarity Trial Results
- Record: found
- Abstract: found
- Article: not found