- Record: found
- Abstract: found
- Article: found
Sequential therapy for 10 days versus triple therapy for 14 days in the eradication of Helicobacter pylori in the community and hospital populations: a randomised trial
Read this article at
Abstract
Objective
Significant heterogeneity was observed in previous trials that assessed the efficacies of sequential therapy for 10 days (S10) versus triple therapy for 14 days (T14) in the first-line treatment of Helicobacter pylori. We aimed to compare the efficacy of S10 and T14 and assess the factors affecting their efficacies.
Design
We conducted this open-label randomised multicentre trial in eight hospitals and one community in Taiwan. 1300 adult subjects with H pylori infection naïve to treatment were randomised (1:1) to receive S10 (lansoprazole and amoxicillin for the first 5 days, followed by lansoprazole, clarithromycin and metronidazole for another 5 days) or T14 (lansoprazole, amoxicillin and clarithromycin for 14 days). All drugs were given twice daily. Successful eradication was defined as negative 13C-urea breath test at least 6 weeks after treatment. Our primary outcome was the eradication rate by intention-to-treat (ITT) and per-protocol (PP) analyses. Antibiotic resistance was determined by agar dilution test.
Results
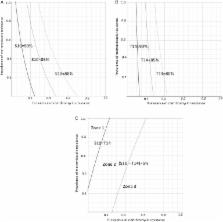
The eradication rates of S10 and T14 were 87.2% (567/650, 95% CI 84.4% to 89.6%) and 85.7% (557/650, 95% CI 82.8% to 88.2%) in the ITT analysis, respectively, and were 91.6% (556/607, 95% CI 89.1% to 93.4%) and 91.0% (548/602, 95% CI 88.5% to 93.1%) in the PP analysis, respectively. There were no differences in compliance or adverse effects. The eradication rates in strains susceptible and resistant to clarithromycin were 90.7% and 62.2%, respectively, for S10, and were 91.5% and 44.4%, respectively, for T14. The efficacy of T14, but not S10, was affected by CYP2C19 polymorphism.
Related collections
Most cited references28
- Record: found
- Abstract: found
- Article: not found
American College of Gastroenterology guideline on the management of Helicobacter pylori infection.
- Record: found
- Abstract: found
- Article: not found