- Record: found
- Abstract: found
- Article: found
Pulmonary embolism as the initial manifestation of right atrial myxoma : A case report and review of the literature
Read this article at
Abstract
Rationale:
Pulmonary embolisms (PEs) are caused by emboli, which mostly originate from deep venous thrombi that travel to and suddenly block the pulmonary arteries. The emboli are usually thrombi, and right atrial myxoma emboli are rare.
Patient concerns:
A 55-year-old man presented with shortness of breath and syncope. We proceeded with computed tomography pulmonary angiography (CTPA) and transthoracic echocardiogram (TTE), the results of which suggested that the diagnosis was a right atrial mass.
Diagnosis:
A definitive diagnosis compatible with a right atrial myxoma (RAM) with tumoral pulmonary emboli after surgical excision was made.
Outcomes:
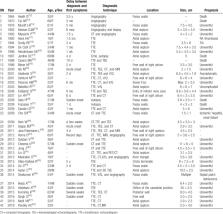
The patient followed an uneventful course during the 6 years of follow-up after surgery. According to a review of the literature, RAMs are often not diagnosed in a timely manner or even go completely undiagnosed. TTE, transesophageal echocardiography (TEE), CT, magnetic resonance imaging (MRI), and positron emission tomography/computed tomography may be helpful in the preoperative diagnosis. Surgical removal of the masses from the atrium and pulmonary arteries was relatively uneventful.
Related collections
Most cited references61
- Record: found
- Abstract: found
- Article: not found
Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases.
- Record: found
- Abstract: found
- Article: not found