- Record: found
- Abstract: found
- Article: found
Measures of Thyroid Function among Belarusian Children and Adolescents Exposed to Iodine-131 from the Accident at the Chernobyl Nuclear Plant
Read this article at
Abstract
Background: Thyroid dysfunction after exposure to low or moderate doses of radioactive iodine-131 ( 131I) at a young age is a public health concern. However, quantitative data are sparse concerning 131I-related risk of these common diseases.
Objective: Our goal was to assess the prevalence of thyroid dysfunction in association with 131I exposure during childhood (≤ 18 years) due to fallout from the Chernobyl accident.
Methods: We conducted a cross-sectional analysis of hypothyroidism, hyperthyroidism, autoimmune thyroiditis (AIT), serum concentrations of thyroid-stimulating hormone (TSH), and autoantibodies to thyroperoxidase (ATPO) in relation to measurement-based 131I dose estimates in a Belarusian cohort of 10,827 individuals screened for various thyroid diseases.
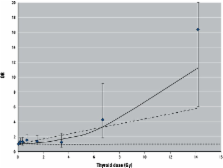
Results: Mean age at exposure (± SD) was 8.2 ± 5.0 years. Mean (median) estimated 131I thyroid dose was 0.54 (0.23) Gy (range, 0.001–26.6 Gy). We found significant positive associations of 131I dose with hypothyroidism (mainly subclinical and antibody-negative) and serum TSH concentration. The excess odds ratio per 1 Gy for hypothyroidism was 0.34 (95% CI: 0.15, 0.62) and varied significantly by age at exposure and at examination, presence of goiter, and urban/rural residency. We found no evidence of positive associations with antibody-positive hypothyroidism, hyperthyroidism, AIT, or elevated ATPO.
Conclusions: The association between 131I dose and hypothyroidism in the Belarusian cohort is consistent with that previously reported for a Ukrainian cohort and strengthens evidence of the effect of environmental 131I exposure during childhood on hypothyroidism, but not other thyroid outcomes.
Related collections
Most cited references43
- Record: found
- Abstract: found
- Article: not found
Subclinical thyroid disease: scientific review and guidelines for diagnosis and management.
- Record: found
- Abstract: found
- Article: not found
The incidence of thyroid disorders in the community: a twenty-year follow-up of the Whickham Survey.
- Record: found
- Abstract: found
- Article: not found