- Record: found
- Abstract: found
- Article: not found
Salivary Detection of COVID-19
other
Lisa Caulley , MD, MPH,
Martin Corsten , MD,
Libni Eapen , MD,
Jonathan Whelan , BSc,
Jonathan B. Angel , MD,
Kym Antonation , MPH,
Nathalie Bastien , PhD,
Guillaume Poliquin , MD, PhD,
Stephanie Johnson-Obaseki , MD, MPH
28 August 2020
Read this article at

There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Background: Standard testing for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
requires a nasopharyngeal or oropharyngeal swab but is limited by modest sensitivity,
the need for health care human resources and personal protective equipment, and the
potential for transmission in transit to or at the testing center. An urgent need
exists for innovative testing strategies to expedite identification of cases and facilitate
mass testing.
Objective: To determine the detection rate of SARS-CoV-2 using a novel, self-administered
kit for saliva collection compared with standard swab testing.
Methods: We prospectively enrolled consecutive, asymptomatic, high-risk persons and
those with mild symptoms suggestive of coronavirus disease 2019 (COVID-19) at a centralized
testing center in Ottawa, Canada. Eligible adults provided 1 saliva specimen using
a self-collection kit (OMNIgene•ORAL, OM-505 [DNA Genotek]) concurrent with their
standard swab test. These kits are designed for self-collection without expert assistance
and can preserve viral material at room temperature for transport and analysis (1).
Total nucleic acid extraction and polymerase chain reaction analysis for SARS-CoV-2
were done at the Eastern Ontario Regional Laboratory in Ottawa for swabs and at the
National Microbiology Laboratory in Winnipeg for saliva. Outcomes were reported for
detection of the SARS-CoV-2 envelope (E) gene with a cycle threshold value less than
37. The Supplement (available at Annals.org) provides additional methodological details.
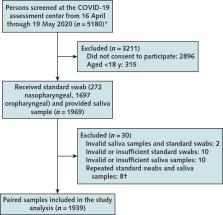
Findings: Of the 1939 paired swab and saliva samples analyzed (Figure), SARS-CoV-2
E gene was detected in 70 samples (Table), 80.0% with swabs and 68.6% with saliva.
Thirty-four participants (48.6%) tested positive for SARS-CoV-2 on both swab and saliva
samples. Discordant test results were seen in 22 participants (31.4%) who tested positive
with swab alone and in 14 (20%) who tested positive with saliva alone. Swabs were
obtained from the nasopharynx in 35.7% of participants who tested positive with saliva
alone, compared with 9.1% of participants who tested positive with swab alone.
Figure.
Study flow diagram.
Standard swab and saliva sample collection during the study period. COVID-19 = coronavirus
disease 2019.
* Inclusion criteria were age ≥18 y, provision of informed consent, and being high-risk
asymptomatic or having mild symptoms of COVID-19. Patients were screened before entry
by a physician. Those with severe symptoms were redirected to an emergency department
for formal clinical evaluation.
† Eight participants were tested twice at the testing center (for both standard swab
and saliva sample). Two tested positive on their initial oropharyngeal swab and negative
on a saliva sample. These participants' results remained positive on an oropharyngeal
swab and negative on a saliva sample on repeated testing (5 d and 8 d later). One
participant tested positive on the initial oropharyngeal swab and negative on the
saliva sample. This participant tested negative on both specimens 7 d later. The remaining
6 participants tested negative on initial and repeated testing for both specimens.
Figure. Study flow diagram. Standard swab and saliva sample collection during the
study period. COVID-19 = coronavirus disease 2019. * Inclusion criteria were age ≥18
y, provision of informed consent, and being high-risk asymptomatic or having mild
symptoms of COVID-19. Patients were screened before entry by a physician. Those with
severe symptoms were redirected to an emergency department for formal clinical evaluation. †
Eight participants were tested twice at the testing center (for both standard swab
and saliva sample). Two tested positive on their initial oropharyngeal swab and negative
on a saliva sample. These participants' results remained positive on an oropharyngeal
swab and negative on a saliva sample on repeated testing (5 d and 8 d later). One
participant tested positive on the initial oropharyngeal swab and negative on the
saliva sample. This participant tested negative on both specimens 7 d later. The remaining
6 participants tested negative on initial and repeated testing for both specimens.
Table. Characteristics of Population That Tested Positive for SARS-CoV-2
Table. Characteristics of Population That Tested Positive for SARS-CoV-2
Discussion: Our study found that standard diagnostic methods of nasopharyngeal and
oropharyngeal swabs detected more COVID-19 cases than saliva testing among patients
who were asymptomatic but at high risk or who were mildly symptomatic. Salivary detection
of SARS-CoV-2 has been proposed as an alternative to standard swab diagnostic methods.
Saliva testing presents potential advantages: Collection does not require trained
staff or personal protective equipment, can be done outside testing centers, and may
be better tolerated in challenging or pediatric populations.
Because of RNA instability, use of raw saliva necessitates rapid transportation to
a laboratory for extraction of viral material and polymerase chain reaction analysis.
This study is unique in that it used a novel collection kit containing a preservative
and viricidal fluid, allowing for safe and stable storage and transport of the samples.
Our findings add to those of previous studies, which have focused on salivary tests
of symptomatic or hospitalized patients (2); these studies have suggested that saliva
tests may be more sensitive. By design, we included asymptomatic and mildly symptomatic
persons to simulate mass screening for COVID-19.
Our study has important limitations. First, evaluating the performance of a novel
diagnostic test in the absence of a true gold standard reference is challenging. The
reported false-negative rate of reverse transcriptase polymerase chain reaction–based
testing for SARS-CoV-2 using swabs is approximately 38% at symptom onset and as high
as 100% shortly after exposure (3). In our study, 20% of COVID-19 cases were detected
by saliva alone, further supporting the notion that standard swab testing may be an
unreliable reference standard. Second, nasopharyngeal or oropharyngeal swabbing was
done according to swab availability at the testing center even though nasopharyngeal
swabs are preferred in symptomatic persons and those later in the illness course (4),
which may have affected our results. Analyses of the influence of swab site on study
results were not done because of limited sample size. Third, analysis of swab and
saliva samples was split between 2 laboratories to accommodate the demand for testing
resources in a pandemic. The potential effect of assay differences was mitigated by
a targeted evaluation of the E gene, a widely accepted and sensitive target gene for
SARS-CoV-2 (5). Finally, more than half of eligible patients declined participation.
Nonetheless, our study shows the feasibility of a simple, safe collection tool for
salivary detection of SARS-CoV-2 in the setting of a COVID-19 testing center. Despite
a lower estimated rate of detection relative to swab testing, saliva testing may be
of particular benefit for remote, vulnerable, or challenging populations.
Supplementary Material
Click here for additional data file.