- Record: found
- Abstract: found
- Article: found
Rat model of veno-arterial extracorporeal membrane oxygenation
Read this article at
Abstract
Background
We aim to develop a rat model of veno-arterial extracorporeal membrane oxygenation (VA-ECMO).
Methods
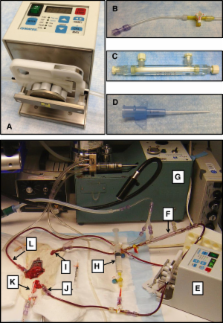
VA-ECMO was established in twelve Male Sprague-Dawley rats (250-350 g) through cannulation of the right jugular vein for venous drainage and the right femoral artery for arterial reinfusion. Arterial blood pressure was measured using a conductance catheter through cannulation of the left carotid artery. Heart rate was monitored by electrocardiography and arterial blood gas parameters with a blood gas analyzer. The VA-ECMO circuit was tested by subjecting the rats to hypoxic cardiac arrest with resuscitation using VA-ECMO. Both load-dependent and load-independent measures of myocardial contractility were measured using pressure-volume loop analysis to confirm restoration of myocardial function post-resuscitation.
Results
Following hypoxic cardiac arrest VA-ECMO provided sufficient oxygenation to support the circulation. The haemodynamic and blood gas parameters were maintained at transition and during ECMO. All animals were resuscitated, regained cardiac function and were able to be weaned off ECMO post-resuscitation.
Related collections
Most cited references5
- Record: found
- Abstract: found
- Article: not found
A 5-year experience with cardiopulmonary resuscitation using extracorporeal life support in non-postcardiotomy patients with cardiac arrest.
- Record: found
- Abstract: found
- Article: not found
Percutaneous venoarterial extracorporeal membrane oxygenation for emergency mechanical circulatory support.
- Record: found
- Abstract: found
- Article: not found