- Record: found
- Abstract: found
- Article: found
A Retrospective Study of thrombolysis with 0.6 mg/kg Recombinant Tissue Plasminogen Activator (rt-PA) in Mild Stroke
Read this article at
Abstract
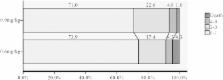
We sought to assess the safety, effectiveness and cost of 0.6 mg/kg rt-PA treatment for patients with acute mild stroke and to compare that with 0.9 mg/kg. We retrospectively analyzed consecutive acute ischemic stroke patients who had a NIHSS score ≤5 at admission and who were treated with rt-PA within 4.5 hours of symptom onset. The demographic data, clinical outcomes and hospitalization cost were analyzed. A total of 108 patients were included. Forty six patients (42.6%) received a 0.6 mg/kg dosage of rt-PA. The baseline characteristics of the two groups were well matched ( p > 0.05). Regarding the safety and effectiveness, the 0.6 mg/kg dosage group had a comparable proportion of symptomatic intracranial hemorrhage (sICH) (0.6 mg/kg, 4.3% vs 0.9 mg/kg, 4.8%; p > 0.05), early neurological deterioration (END) (19.6% vs 17.7%; p > 0.05), in-hospital mortality (4.3% vs 1.6%; p > 0.05), and a similar rate of favorable functional outcome (mRS score 0–1) at 3 months (73.9% vs 71.0%; p > 0.05) to those who received the standard dosage. However, the hospital cost was markedly lower in the 0.6 mg/kg group (0.6 mg/kg, 3,401.7 USD vs 0.9 mg/kg, 4,157.4 USD; p < 0.01). Our study suggest that 0.6 mg/kg rt-PA shared similar effectiveness and safety profile compared with that of 0.9 mg/kg in treating mild stroke, but cost less.
Related collections
Most cited references20
- Record: found
- Abstract: found
- Article: not found
What is a minor stroke?
- Record: found
- Abstract: found
- Article: not found
Alteplase at 0.6 mg/kg for acute ischemic stroke within 3 hours of onset: Japan Alteplase Clinical Trial (J-ACT).
- Record: found
- Abstract: found
- Article: not found