- Record: found
- Abstract: found
- Article: not found
Acupuncture and other physical treatments for the relief of pain due to osteoarthritis of the knee: network meta-analysis ☆
Read this article at

Summary
Objective
To compare the effectiveness of acupuncture with other relevant physical treatments for alleviating pain due to knee osteoarthritis.
Design
Systematic review with network meta-analysis, to allow comparison of treatments within a coherent framework. Comprehensive searches were undertaken up to January 2013 to identify randomised controlled trials in patients with osteoarthritis of the knee, which reported pain.
Results
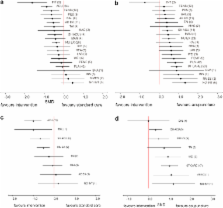
Of 156 eligible studies, 114 trials (covering 22 treatments and 9,709 patients) provided data suitable for analysis. Most trials studied short-term effects and many were classed as being of poor quality with high risk of bias, commonly associated with lack of blinding (which was sometimes impossible to achieve). End of treatment results showed that eight interventions: interferential therapy, acupuncture, TENS, pulsed electrical stimulation, balneotherapy, aerobic exercise, sham acupuncture, and muscle-strengthening exercise produced a statistically significant reduction in pain when compared with standard care. In a sensitivity analysis of satisfactory and good quality studies, most studies were of acupuncture (11 trials) or muscle-strengthening exercise (9 trials); both interventions were statistically significantly better than standard care, with acupuncture being statistically significantly better than muscle-strengthening exercise (standardised mean difference: 0.49, 95% credible interval 0.00–0.98).
Conclusions
As a summary of the current available research, the network meta-analysis results indicate that acupuncture can be considered as one of the more effective physical treatments for alleviating osteoarthritis knee pain in the short-term. However, much of the evidence in this area of research is of poor quality, meaning there is uncertainty about the efficacy of many physical treatments.
Related collections
Most cited references19
- Record: found
- Abstract: found
- Article: not found
OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines.
- Record: found
- Abstract: found
- Article: not found
Interpreting the clinical importance of group differences in chronic pain clinical trials: IMMPACT recommendations.
- Record: found
- Abstract: found
- Article: not found