- Record: found
- Abstract: found
- Article: found
Bakers' cyst and tibiofemoral abnormalities are more distinctive MRI features of symptomatic osteoarthritis than patellofemoral abnormalities
Read this article at
Abstract
Objective
To investigate which structural MR abnormalities discriminate symptomatic knee osteoarthritis (OA), taking co-occurrence of abnormalities in all compartments into account.
Methods
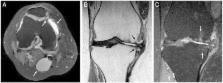
The Netherlands Epidemiology of Obesity (NEO) study is a population-based cohort aged 45–65 years. In 1285 participants (median age 56 years, 55% women, median body mass index (BMI) 30 kg/m 2), MRI of the right knee were obtained. Structural abnormalities (osteophytes, cartilage loss, bone marrow lesions (BMLs), subchondral cysts, meniscal abnormalities, effusion, Baker's cyst) at 9 patellofemoral and tibiofemoral locations were scored following the knee OA scoring system. Symptomatic OA in the imaged knee was defined following the American College of Rheumatology criteria. Logistic ridge regression analyses were used to investigate which structural abnormalities discriminate best between individuals with and without symptomatic OA, crude and adjusted for age, sex and BMI.
Results
Symptomatic knee OA was present in 177 individuals. Structural MR abnormalities were highly frequent both in individuals with OA and in those without. Baker's cysts showed the highest adjusted regression coefficient (0.293) for presence of symptomatic OA, followed by osteophytes and BMLs in the medial tibiofemoral compartment (0.185–0.279), osteophytes in the medial trochlear facet (0.262) and effusion (0.197).
Related collections
Most cited references23
- Record: found
- Abstract: found
- Article: not found
The association of bone marrow lesions with pain in knee osteoarthritis.
- Record: found
- Abstract: found
- Article: not found
Osteoarthritis of the knee: association between clinical features and MR imaging findings.
- Record: found
- Abstract: found
- Article: not found