- Record: found
- Abstract: found
- Article: found
Preincisional administration of intravenous or subcutaneous infiltration of low-dose ketamine suppresses postoperative pain after appendectomy
Abstract
Background
Ketamine, an N-methyl-D-aspartate receptor antagonist, can suppress hyperalgesia and allodynia. The purpose of the present study was to evaluate the clinical efficacy of preincisional intravenous or subcutaneous infiltration of ketamine for postoperative pain relief after appendectomy.
Methods
Ninety patients, aged 18–60 years, scheduled for appendectomy was enrolled in this study. Patients were divided into three groups of 30 each and received subcutaneous infiltration of ketamine 0.5 mg/kg (KS), intravenous ketamine 0.5 mg/kg (KI), or subcutaneous infiltration of normal saline 3 mL (C) before surgery. Visual analog scale (VAS) values and analgesic consumption were evaluated for 24 hours after surgery.
Results
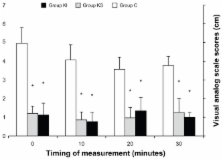
VAS scores were significantly lower at the time of arrival in the recovery room, and at 10, 20, and 30 minutes thereafter in group KI and group KS compared with group C ( P < 0.05). VAS scores were not significantly different between group KI and group KS at these intervals. Postoperative VAS scores were significantly lower at 6, 12, 18, and 24 hours in group KI compared with group C ( P < 0.05). In group KS, the postoperative VAS score was significantly lower at 6 hours ( P < 0.05). VAS scores were significantly lower at 12, 18, and 24 hours after surgery in group KI compared with group KS ( P < 0.05).
Most cited references26
- Record: found
- Abstract: found
- Article: not found
Ketamine and postoperative pain--a quantitative systematic review of randomised trials.
- Record: found
- Abstract: found
- Article: not found
Intraoperative ketamine reduces perioperative opiate consumption in opiate-dependent patients with chronic back pain undergoing back surgery.
- Record: found
- Abstract: found
- Article: not found