- Record: found
- Abstract: found
- Article: found
Reemerging Ebola haemorrhagic fever 2014 and the risks of its introduction into Brazil
editorial
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
The Ebola virus was identified in 1976 during epidemics of haemorrhagic fever in southern
Sudan and northern Zaire (now the Democratic Republic of the Congo). The average mortality
rate of Ebola virus disease, formerly known as Ebola haemorrhagic fever, is around
50% with
rates varying from 25-90% in past outbreaks. The chronology of the outbreaks of the
disease
in different countries since 1976, according to the virus subtypes, numbers of cases
and
notified deaths up to November 2014 can be seen in Table. In this latest epidemic,
eight countries have been affected: Guinea,
Liberia and Sierra Leone have been the most affected countries while cases have been
recorded in Nigeria, Senegal, United States of America (USA), Spain and Mali. A separate,
unrelated Ebola outbreak occurred in Boende, Equateur, an isolated part of the Democratic
Republic of Congo in August-October 2014.
TABLE
Outbreaks chronology of Ebola virus disease
Years/months
Countries/area
Subtypes of Ebola
Cases (n)
Total of death n
(%)
1976
Congo DRC
Zaire virus
318
280 (88)
1976
South Sudan
Sudan virus
284
151 (53)
1977
Congo DRC
Zaire virus
1
1 (100)
1979
South Sudan
Sudan virus
34
22 (65)
1994
Gabon
Zaire virus
52
31 (60)
1995
Congo DRC
Zaire virus
315
250 (81)
1996 January-April
Gabon
Zaire virus
37
21 (57)
1996 July-1997 January
Gabon
Zaire virus
60
45 (74)
2000-2001
Uganda
Sudan virus
425
224 (53)
2001 October-2002 March
Gabon
Zaire virus
65
53 (82)
2001 October-2002 March
Congo DRC
Zaire virus
57
43 (75)
2002 December-2003 April
Congo DRC
Zaire virus
143
128 (89)
2003 November-December
Congo DRC
Zaire virus
35
29 (83)
2004
South Sudan
Sudan virus
17
7 (41)
2007
Congo DRC
Zaire virus
264
187 (71)
2007 December-2008 January
Uganda
Bundibugyo virus
149
37 (25)
2008 December-2009 February
Congo DRC
Zaire virus
32
15(47)
2011 May
Uganda
Sudan virus
1
1 (100)
2012 June-October
Uganda
Sudan virus
11
4 (36)
2012 June-November
Congo DRC
Bundibugyo virus
36
13 (36)
2012 November-2013 January
Uganda
Sudan virus
6
3 (50)
2014 August-October
Congo DRC
Zaire virus
66
49 (74)
2014 March-28 November
Mainly West Africa
a
Zaire virus
15,935
5,689 (36)
a: Guinea, Liberia and Sierra Leone have been the most
affected countries while cases have been recorded in Nigeria, Senegal, the
United States of America (USA), Spain and Mali. Senegal and Nigeria were
declared free of Ebola infection by World Health Organization in October 2014.
From 1976-2014, about 15 cases of human infection with Ebola virus from monkeys
imported cases or laboratory accident of scientists and health workers occurred
in USA, England, Italy, South Africa and Russia.
Filoviral diseases are caused by viruses of the family Filoviridae, which is composed
by
the Marburg, Cueva and Ebola viruses. Filoviruses are particles formed by long filaments
that contain a single strand of RNA and they cause haemorrhagic fever in humans and
non-human primates (monkeys, gorillas and chimpanzees). Given the lethal nature of
these
viruses, they are considered to be class IV pathogens, i.e., highly dangerous. Five
subtypes of the Ebola virus have been identified: Zaire Ebola virus, Reston Ebola
virus,
Sudan Ebola virus, Tai Forest Ebola virus and Bundibugyo Ebola virus (Figure). The
Zaire, Sudan and Bundibugyo subtypes have been responsible
for major outbreaks of the disease. On the other hand, although the Reston and Tai
Forest
subtypes may affect human beings, no cases of fever and death among humans have been
notified.
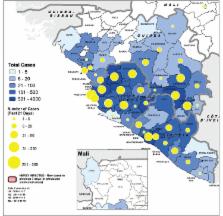
Geographical distribution of probable and confirmed cases in the past 21 days
and total cases in Guinea, Liberia, Mali and Sierra Leone. Source: World Health
Organization 2014 (dated 21 November). Ebola Response Roadmap Situation
Report Update.
The hosts of the Ebola virus are fruit-eating bats of the family Pteropodidae. Introduction
of the virus into the human population occurs through close contact with blood, secretions,
organs and other fluids from infected animals such as chimpanzees, gorillas, fruit-eating
bats, monkeys, wild antelopes and wild pigs that are found sick or dead in the rainforests.
The Ebola virus is transmitted among human beings through direct contact by means
of
lacerated skin or mucosa, with blood, secretions, organs and other body fluids from
infected individuals or by means of materials and clothing that have become contaminated
with these fluids.
Healthcare professionals (physicians, nurses, pathologists and researchers) often
become
infected when they are treating patients with suspected or confirmed Ebola virus infection,
through direct contact. A total of 558 healthcare workers are known to have been infected
in the current outbreak of which 337 have died (data up to 21 November 2014). Furthermore,
laboratory accidents and research activities on the virus in human beings and animals
may
give rise to the risk of infection, when precautions are not rigorously maintained.
Individuals remain infected with the virus in their blood and body fluids, including
semen
and breast milk. After recovery from the disease, men can still transmit the virus
through
their semen for seven weeks after the disease.
The incubation period for the disease, between penetration of the virus and the start
of
symptoms, is from two-21 days. The first symptoms are sudden fever and fatigue, muscle
pain, headache and sore throat. These symptoms are followed by vomiting, diarrhoea,
skin
rashes, kidney and liver impairment and, in some cases, internal and external bleeding,
such as through the gums and in the faeces. The most frequent laboratory findings
are
diminished platelet levels and elevation of hepatic enzymes.
In making the diagnosis, it may be difficult to distinguish between infections due
to the
Ebola virus and due to other diseases such as malaria, typhoid fever and
meningoencephalitis. Ebola infection can be confirmed through the following investigations:
(i) presence of antibodies seen through ELISA, (ii) detection through antigen uptake,
(iii)
serological neutralisation test, (iv) electron microscopy and (v) isolation of the
virus
through culturing. Samples of material from patients are extremely infectious and
the
laboratory tests have to be performed under the highest safety conditions, both for
the
technician and for the other people who use the laboratory.
The treatment should consist of support: oral or intravenous rehydration and treatment
of
the symptoms. There is still no specific treatment, but drugs that have been shown
to be
specific when used on sick animals are being tested experimentally on humans. Treatment
using serum from patients who have been cured of the disease have been promising.
Three
research projects will take place in West Africa, testing antiviral drugs and the
use of
survivors’ blood to treat the sick. No licensed vaccine is available, but two potential
vaccines are being tested on humans.
Prevention and control of the disease is currently based on isolating the patients,
absolute protection for the healthcare professionals who are caring for the patients
and
quarantine for individuals who have come into close contact with patients, including
members of their families.
Risk of introduction of the Ebola virus into Brazil - Brazil has a coastal
frontier of 7,367 km and its terrestrial limits are its borders with 10 other South
American countries (Argentina, Bolivia, Colombia, Guyana, French Guiana, Paraguay,
Peru,
Suriname, Uruguay and Venezuela) with a total length of the order of 16,886 km. Thus,
this
is a very extensive terrestrial border along which it is difficult to control the
entry of
people from other countries. This is particularly so in relation to the countries
that
border the Brazilian Amazon Region: Bolivia, Colombia, Guyana, French Guiana, Suriname,
Peru and Venezuela. On the other hand, more than 25 ports and 20 international airports
open up Brazil to the whole world, not only by means of maritime and air transport
directly
between Brazil and Africa, but also particularly from African countries to Europe
and other
continents and from there to Brazil. According to the World Tourism Organization,
in 2012
Brazil received 5.6 million visitors (2014 estimate 6.4 million), however no African
country was among the top 20 sending countries.
A study conducted by the Biological System Modeling Laboratory of Northeastern University
in the USA, in September 2014, investigated the risk associated with the Ebola outbreak
in
West Africa in 2014 (Sierra Leone, Guinea, Liberia and Nigeria). The study covered
220
countries and Brazil was in 30th place, with a 5% risk of importing the virus by 31
October
2014. This represented a high short-term risk. It is to be hoped that this prediction
does
not become a reality, but preparations need to be made for such an emergency, until
such
time that the World Health Organization considers that the epidemic in West Africa
or in
any other country has been brought under control.
Given the long incubation period of the disease, it is recognised that it is not an
easy
task to avoid the entry of individuals who are still in the asymptomatic phase or
to detect
symptomatic individuals at ports, airports and especially at the terrestrial borders,
particularly those with countries in the Amazon Region. Nonetheless, in the light
of this
emergency regarding the possibility of introduction of the Ebola virus into Brazil,
integrated surveillance measures are being introduced by the Ministries of Health,
Justice
and Foreign Relations at Brazil’s borders in relation to individuals with possible
Ebola
virus infection, as follows: (i) detailed review of documentation regarding the origin
of
passengers arriving at terrestrial, port and airport borders, (ii) establishment of
brief
questionnaires about countries visited over the preceding 30 days and any manifestations
of
symptoms that may have resulted from Ebola virus infection, (iii) review of the quarantine
law in relation to individuals with suspected Ebola disease, (iv) guidance from the
Foreign
Ministry for Brazilian citizens who live in countries that are at risk of Ebola disease
and
for those who come from abroad to Brazil and, lastly, (v) the Ministry of Health has
the
responsibility for surveillance and medical healthcare for suspected or confirmed
cases of
this disease.
In addition to the formal recommendations that the Ministry of Health has been making
with
regard to surveillance at ports and airports, we suggest that it should make further
recommendations to all Brazilian state health departments for preparations for medical
care
in suspected or confirmed cases of this disease. Given the size of Brazil, it is impossible
to predict when the disease might enter the country and it becomes difficult to conduct
centralised laboratory tests in Belém, state of Pará (no matter how competent the
laboratory is) and to provide medical care at a single hospital in Rio de Janeiro
(the
current scenario). We suggest to the Ministry of Health to take the following measures:
(i)
set up a task force of physicians and senior nurses with the capacity to train teams
within
state health departments, regarding surveillance and medical care for patients with
suspected or confirmed Ebola virus infection, (ii) help in setting up and training
for
diagnostic and medical care centres for this disease, within state health departments
and
(ii) maintain surveillance at the diagnostic and medical care centres of state health
departments through retraining their teams, when necessary.
José Rodrigues Coura
Hooman Momen
Associated EditorsMemórias do Instituto Oswaldo Cruz
Related collections
Author and article information
Comments
Comment on this article
scite_