- Record: found
- Abstract: found
- Article: found
Alveolar–capillary reserve during exercise in patients with chronic obstructive pulmonary disease
Abstract
Background
Factors limiting exercise in patients with COPD are complex. With evidence for accelerated pulmonary vascular aging, destruction of alveolar–capillary bed, and hypoxic pulmonary vasoconstriction, the ability to functionally expand surface area during exercise may become a primary limitation.
Purpose
To quantify measures of alveolar–capillary recruitment during exercise and the relationship to exercise capacity in a cohort of COPD patients.
Methods
Thirty-two subjects gave consent (53% male, with mean ± standard deviation age 66±9 years, smoking 35±29 pack-years, and Global Initiative for Chronic Obstructive Lung Disease (GOLD) classification of 0–4: 2.3±0.8), filled out the St George’s Respiratory Questionnaire (SGRQ) to measure quality of life, had a complete blood count drawn, and underwent spirometry. The intrabreath (IB) technique for lung diffusing capacity for carbon monoxide (IBDLCO) and pulmonary blood flow (IBQc, at rest) was also performed. Subsequently, they completed a cycle ergometry test to exhaustion with measures of oxygen saturation and expired gases.
Results
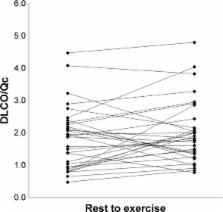
Baseline average measures were 44±21 for SGRQ score and 58±11 for FEV 1/FVC. Peak oxygen consumption (VO 2) was 11.4±3.1 mL/kg/min (49% predicted). The mean resting IBDLCO was 9.7±5.4 mL/min/mmHg and IBQc was 4.7±0.9 L/min. At the first workload, heart rate (HR) increased to 92±11 bpm, VO 2 was 8.3±1.4 mL/kg/min, and IBDLCO and IBQc increased by 46% and 43%, respectively, compared to resting values ( p,0.01). The IBDLCO/Qc ratio averaged 2.0±1.1 at rest and remained constant during exercise with marked variation across subjects (range: 0.8–4.8). Ventilatory efficiency plateaued at 37±5 during exercise, partial pressure of mix expired CO 2/partial pressure of end tidal CO 2 ratio ranged from 0.63 to 0.67, while a noninvasive index of pulmonary capacitance, O 2 pulse × PetCO 2 (GxCap) rose to 138%. The exercise IBDLCO/Qc ratio was related to O 2 pulse (VO 2/HR, r=0.58, p<0.01), and subjects with the highest exercise IBDLCO/Qc ratio or the greatest rise from rest had the highest peak VO 2 values ( r=0.65 and 0.51, respectively, p<0.05). Of the noninvasive gas exchange measures of pulmonary vascular function, GxCap was most closely associated with DLCO, DLCO/Qc, and VO 2 peak.
Most cited references27
- Record: found
- Abstract: found
- Article: not found
Pulmonary hypertension in chronic lung diseases.
- Record: found
- Abstract: found
- Article: not found
Exercise pathophysiology in patients with primary pulmonary hypertension.
- Record: found
- Abstract: not found
- Article: not found