- Record: found
- Abstract: found
- Article: found
Myocardial scarring on cardiovascular magnetic resonance in asymptomatic or minimally symptomatic patients with “pure” apical hypertrophic cardiomyopathy
Read this article at
Abstract
Background
Late gadolinium enhancement (LGE) cardiovascular magnetic resonance (CMR) enables state-of-the-art in vivo evaluations of myocardial fibrosis. Although LGE patterns have been well described in asymmetrical septal hypertrophy, conflicting results have been reported regarding the characteristics of LGE in apical hypertrophic cardiomyopathy (ApHCM). This study was undertaken to determine 1) the frequency and distribution of LGE and 2) its prognostic implication in ApHCM.
Methods
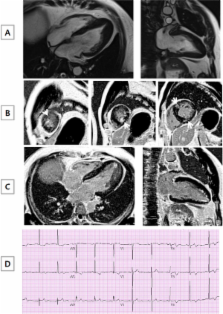
Forty patients with asymptomatic or minimally symptomatic pure ApHCM (age, 60.2 ± 10.4 years, 31 men) were prospectively enrolled. LGE images were acquired using the inversion recovery segmented spoiled-gradient echo and phase-sensitive inversion recovery sequence, and analyzed using a 17-segment model. Summing the planimetered LGE areas in all short axis slices yielded the total volume of late enhancement, which was subsequently presented as a proportion of total LV myocardium (% LGE).
Results
Mean maximal apical wall thickness was 17.9±2.3mm, and mean left ventricular (LV) ejection fraction was 67.7 ± 8.0%. All but one patient presented with electrocardiographic negative T wave inversion in anterolateral leads, with a mean maximum negative T wave of 7.2 ± 4.7mm. Nine patients (22.5%) had giant negative T waves, defined as the amplitude of ≥10mm, in electrocardiogram. LGE was detected in 130 segments of 30 patients (75.0%), occupying 4.9 ± 5.5% of LV myocardium. LGE was mainly detected at the junction between left and right ventricles in 12 (30%) and at the apex in 28 (70%), although LGE-positive areas were widely distributed, and not limited to the apex. Focal LGE at the non-hypertrophic LV segments was found in some ApHCM patients, even without LGE of hypertrophied apical segments. Over the 2-year follow-up, there was no one achieving the study end-point, defined as all-cause death, sudden cardiac death and hospitalization for heart failure.
Related collections
Most cited references22
- Record: found
- Abstract: found
- Article: not found
Hypertrophic cardiomyopathy: a systematic review.
- Record: found
- Abstract: found
- Article: not found
Delayed enhancement cardiovascular magnetic resonance assessment of non-ischaemic cardiomyopathies.
- Record: found
- Abstract: found
- Article: not found