- Record: found
- Abstract: found
- Article: found
Prevalence of undiagnosed airflow obstruction among people with a history of smoking in a primary care setting
Abstract
Purpose
The purpose of this study was to define the prevalence of undiagnosed airflow obstruction (AO) among subjects with a history of smoking but no previous diagnosis of chronic lung disease. The finding of AO likely represents diagnosis of chronic obstructive pulmonary disease.
Patients
People aged ≥30 years with a history of smoking who attended public outpatient clinics for primary care services were included in this study.
Methods
A cross-sectional survey in five clinics in Hong Kong using the Breathlessness, Cough, and Sputum Scale, the Lung Function Questionnaire, and office spirometry was conducted.
Results
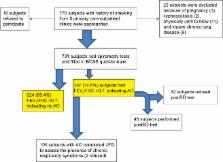
In total, 731 subjects (response rate =97.9%) completed the questionnaires and spirometry tests. Most of the subjects were men (92.5%) in the older age group (mean age =62.2 years; standard deviation =11.7). Of the 731 subjects, 107 had AO, giving a prevalence of 14.6% (95% confidence interval =12.1–17.2); 45 subjects with AO underwent a postbronchodilator test. By classifying the severity of chronic obstructive pulmonary disease using the Global Initiative for Chronic Obstructive Lung Disease, 27 (60%) were considered to be in mild category and 18 (40%) in moderate category. None of them belonged to the severe or very severe category. The total score of Lung Function Questionnaire showed that majority of the subjects with AO also had chronic cough, wheezing attack, or breathlessness, although most did not show any acute respiratory symptoms in accordance with the Breathlessness, Cough, and Sputum Scale. Diagnosis of AO was positively associated with the number of years of smoking (odds ratio =1.044, P=0.035) and being normal or underweight (odds ratio =1.605, P=0.046). It was negatively associated with a history of hypertension (odds ratio =0.491, P=0.003).
Most cited references26
- Record: found
- Abstract: found
- Article: not found
The natural history of chronic airflow obstruction.
- Record: found
- Abstract: found
- Article: not found
Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1. The Lung Health Study.
- Record: found
- Abstract: found
- Article: not found