- Record: found
- Abstract: found
- Article: found
Ablation of ventricular tachycardia from the aortic root after transcatheter aortic valve replacement
case-report
Uma N. Srivatsa , MBBS, MAS, FHRS
∗ ,
Eric J. Nordsieck , MD,
Nayereh Pezeshkian , MD, MPH, FHRS,
Yingbo Yang , MD,
Jeffrey Southard , MD
14 March 2018
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Introduction
Key Teaching Points
•
Iatrogenic ventricular tachycardia can occur after transcatheter aortic valve replacement.
•
The mechanism of this ventricular tachycardia likely is trigger or automaticity.
•
Ablation is safely possible between the valve strut and the sinus of Valsalva.
Transcatheter aortic valve replacement (TAVR) is an increasingly common procedure
for treatment of patients with severe symptomatic aortic stenosis who are at intermediate
to high risk for traditional surgical valve replacement. Although conduction disturbances
and the need for pacemaker implantation postprocedure are well-recognized complications,
ventricular arrhythmias (VAs) have not been widely reported. We present a case of
focal outflow tract tachycardia occurring late post-TAVR accessible from the left
coronary cusp (LCC)/noncoronary cusp junction adjacent to the valve strut, which was
treated successfully with radiofrequency (RF) ablation.
Case report
A 78-year-old Caucasian man with diabetes, hypertension, and previous coronary artery
bypass surgery presented with complaints of progressive dyspnea on exertion and was
found to have severe aortic valve stenosis. Transthoracic echocardiography revealed
preserved left ventricular (LV) ejection fraction, with an estimated valve area of
0.8 cm2 and mean gradient of 40 mm Hg. Because of the high surgical risk associated
with redo sternotomy, the patient underwent successful transfemoral TAVR with a 26-mm
Edwards SAPIEN valve (Edwards Lifesciences Corp, Irvine, CA), which resulted in improved
symptoms and function. However, 3 years later, he complained of fatigue and palpitations.
Electrocardiography showed frequent premature ventricular contractions (PVCs), and
24-hour monitoring revealed high PVC burden (53% of total beats) and 368 runs of nonsustained
ventricular tachycardia. The patient did not improve on medical therapy with beta-blocker.
Repeat transthoracic echocardiography showed interval dilation of the LV and a reduction
in LV ejection fraction from 65% to 55%. PVC morphology suggested left ventricular
outflow tract (LVOT) origin (Figure 1A) based on QS pattern in leads aVR and aVL,
rS in lead V1, and inferior axis in leads II, III, and aVF. The patient was referred
for ablation of symptomatic PVCs. A 3.5-mm NaviStar ThermoCool RMT catheter (Biosense
Webster Inc, Diamond Bar, CA) was advanced in retrograde aortic fashion to the ascending
aorta via femoral arterial access. Intracardiac echocardiography was used to monitor
valve function and visualize the valve struts and the sinuses of Valsalva (Figure 1B).
A stereotaxis magnetic navigational system was used to advance the catheter through
the TAVR bioprosthesis and map the LV. Irregularity of coupling intervals between
PVCs and the preceding QRS complexes was noted, suggesting a nonreentrant mechanism.
Electrophysiologic study and mapping with the CARTO system (Biosense Webster) identified
earliest activation of the PVCs in the LVOT at the site of a focal area of scar at
the septal end of the LCC (Figures 1C and 2A, left). Using stereotaxis magnetic navigation,
the catheter was positioned into the cusp junction between the valve strut and the
sinus of Valsalva (Figure 2B). Pace-mapping performed at this location (2-ms pulse
width and lowest captured output) revealed a 98% match to the clinical PVCs (Figure
2A, middle). After the safety of the location was confirmed by coronary angiography,
focal ablation was initiated at 25 W and titrated up to 35 W for an average delivery
of 33 W (Figure 2A, right, and 2B). PVCs were eliminated within 1.2 seconds, and ablation
was delivered for a total 90 seconds. Postablation intracardiac echocardiographic
imaging revealed no damage to the aortic valve apparatus, and PVCs could not be reinduced
by pacing or isoprenaline administration. At 2-year follow-up, the patient has improved
symptoms and no recurrence of PVCs.
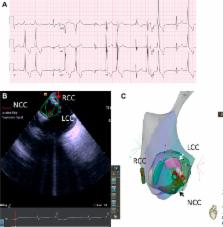
Figure 1
A: Baseline 12-lead electrocardiogram reveals frequent premature ventricular complexes
of left bundle branch morphology. B, C: Images of the left ventricular outflow tract
(LVOT). Cusps are labeled. B: Intracardiac echocardiography. Green lines represent
valve cusps. Red arrow indicates the valve strut. Red ablation tags (white location
tags) are seen at the septal end of LCC. C: CARTO sound image of the LVOT. White arrow
and black arrow indicate LCC and NCC, respectively. The ablation catheter can be seen.
LCC = left coronary cusp; NCC = noncoronary cusp; RCC = right coronary cusp.
Figure 2
A: Activation mapping of the left ventricular outflow tract (LVOT). Left: Earliest
activation spot on the intracardiac electrogram is seen at –116 ms. Middle: Pace-map.
Right: Ablation spot. B: Fluoroscopic image of the LVOT in an anteroposterior view.
Edwards SAPIEN 3 valve struts are seen. Ablation catheter is located between the struts
and the left sinus of Valsalva.
Discussion
VAs occurring post-TAVR are not commonly reported despite the increasing prevalence
of the procedure. The feasibility and safety of RF ablation in the coronary sinuses
or LVOT after TAVR have not been reported. The previous case reported in the literature
was also suspected to be of LVOT origin based on surface ECG morphology but was treated
medically without further evaluation by invasive electrophysiologic study.
1
Here we report a successful case of RF ablation from the left coronary sinus of Valsalva,
behind the TAVR valve strut, assisted by intracardiac echocardiography and a magnetic
catheter navigation system.
VAs arising from the outflow tracts in structurally normal hearts are thought to be
attributable to triggered activity; however, even in structural heart disease, nonreentrant
mechanisms of outflow tract VA are not uncommon.2, 3 Conduction disturbances post-TAVR
are well-recognized complications and speculated to be due to local tissue injury
of the proximal His–Purkinje system in the intraventricular septum.
4
In the patient reported here, the development of VA occurred several years after TAVR
placement and therefore was not due to acute tissue injury. The origin of the PVC
is inconsistent with the right coronary cusp based on rS in lead V1 but is suggestive
of an LCC origin based on the amplitude of leads II/III, although R in lead II is
slightly taller in our case.
5
We localized the PVC to the LCC on the septal end by activation mapping. The presence
of a small focal scar was noted at the site of PVC localization, which may be consistent
with remote injury. Early study of patients with aortic stenosis revealed a higher
prevalence of PVCs, which was not lowered after surgical aortic valve replacement.
6
Ventricular tachycardia after surgical aortic valve replacement has been shown to
be due to reentry, bundle branch reentry, or triggered activity, and ablation has
been successfully performed in these situations.7, 8, 9, 10 In our case, the varying
coupling intervals and rapid success of point ablation are suggestive of triggered
activity or abnormal automaticity as a possible mechanism.
Conclusion
We report the first case of successful RF ablation of frequent focal LVOT PVCs from
the LCC adjacent to the TAVR valve. Placement of the ablation catheter into the sinuses
of Valsalva adjacent to the valve struts in post-TAVR patients is feasible, without
causing damage to percutaneously placed aortic valve prostheses.
Related collections
Most cited references9
- Record: found
- Abstract: found
- Article: not found
Sustained ventricular tachycardia associated with corrective valve surgery.
Robert Eckart, Tomasz Hruczkowski, Bruce A. Koplan … (2007)
- Record: found
- Abstract: found
- Article: not found
Ventricular tachycardia in valvular heart disease: facilitation of sustained bundle-branch reentry by valve surgery.
Laxmikant S. Deshpande, Z Blanck, A Dhala … (1997)