- Record: found
- Abstract: found
- Article: found
Systematic review of public health research on prevention of mother-to-child transmission of HIV in India with focus on provision and utilization of cascade of PMTCT services
Read this article at
Abstract
Background
In spite of effective strategies to eliminate mother-to-child-transmission of HIV, the implementation of such strategies remains a major challenge in developing countries. In India, programs for the prevention of mother-to-child transmission (PMTCT) have been scaled up widely since 2005. However, these programs reach only a small percentage of pregnant women, and their overall effectiveness is low. Evidence-based program planning and implementation could significantly improve their effectiveness. This study sought to systematically retrieve, thematically categorize and review published research on PMTCT of HIV in India, focusing on research related to the provision and/or utilization of the cascade of services provided in a PMTCT program, in order to direct further research to enhance program implementation and effectiveness.
Methods
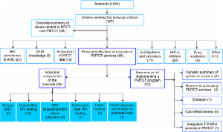
A systematic search using MEDLINE, US National Library of Medicine Gateway system (PubMed) and ISI Web of Knowledge resulted in 1,944 abstracts, of which 167 met our inclusion criteria.
Results
A huge share of the empirical literature on PMTCT in India (N = 134) deals with epidemiological studies (N = 60). The 46 papers related to utilization/provision of the cascade of PMTCT services were mostly from the four high HIV prevalence states in southern India and from the public sector. Studies on experiences of implementing a PMTCT program (N = 20) show high rates of drop out of women in the cascade particularly prior to receiving ARV. Studies on individual components of the cascade (N = 26) show that HIV counseling and testing is acceptable and feasible. Literature on other components of the cascade - such as pregnant women’s access to ANC care, HIV infected women’s immunological assessment using CD4 testing, repeat HIV testing among pregnant women, early infant diagnosis and factors related to linking HIV infected women and children to postnatal care – is lacking.
Conclusions
While the scale of the Indian PMTCT program is large, comprehensive understanding of the context-driven factors affecting its efficiency is lacking. Systematic and more focused public health research output is needed on the issues related to reduction of drop outs of women in the cascade, role of PMTCT programs in improving maternal and child health indicators and role of private sector in delivering PMTCT services.
Related collections
Most cited references60
- Record: found
- Abstract: found
- Article: not found
Combination antiretroviral strategies for the treatment of pregnant HIV-1-infected women and prevention of perinatal HIV-1 transmission.
- Record: found
- Abstract: found
- Article: not found