- Record: found
- Abstract: found
- Article: found
Comparison of Percutaneous Endoscopic Lumbar Discectomy with Minimally Invasive Transforaminal Lumbar Interbody Fusion as a Revision Surgery for Recurrent Lumbar Disc Herniation after Percutaneous Endoscopic Lumbar Discectomy
Abstract
Objective
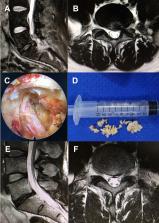
The purpose of this study was to compare the outcomes between percutaneous endoscopic lumbar discectomy (PELD) and minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) for the revision surgery for recurrent lumbar disc herniation (rLDH) after PELD surgery.
Patients and Methods
A total of 46 patients with rLDH were retrospectively assessed in this study. All the patients had received a PELD in Peking University First Hospital between January 2015 and June 2019, before they underwent a revision surgery by either PELD (n=24) or MIS-TLIF (n=22). The preoperative data, perioperative conditions, complications, recurrence condition, and clinical outcomes of the patients were compared between the two groups.
Results
Compared to the MIS-TLIF group, the PELD group had significantly shorter operative time, less intraoperative hemorrhage, and shorter postoperative hospitalization, but higher recurrence rate ( P<0.05). Complication rates were comparable between the two groups. Both groups had satisfactory clinical outcomes at a 12-month follow-up after the revision surgery. The PELD group also showed significantly lower visual analog scale (VAS) scores of back pain and Oswestry disability index (ODI) in one month after the revision surgery, whereas the difference was not detectable at six- and 12-month follow-ups.
Conclusion
Both PELD and MIS-TLIF are effective as a revision surgery for rLDH after primary PELD. PELD is superior to MIS-TLIF in terms of operative time amount of intraoperative hemorrhage and postoperative hospitalization. However, its higher postoperative recurrence rate must be considered and patients should be well informed, when making a decision between the two surgical approaches.
Most cited references47
- Record: found
- Abstract: found
- Article: not found
Transforaminal posterolateral endoscopic discectomy with or without the combination of a low-dose chymopapain: a prospective randomized study in 280 consecutive cases.
- Record: found
- Abstract: found
- Article: not found
Posterolateral endoscopic excision for lumbar disc herniation: Surgical technique, outcome, and complications in 307 consecutive cases.
- Record: found
- Abstract: found
- Article: not found