- Record: found
- Abstract: found
- Article: found
Simultaneous 13N-Ammonia and gadolinium first-pass myocardial perfusion with quantitative hybrid PET-MR imaging: a phantom and clinical feasibility study

Read this article at
Abstract
Background
Positron emission tomography (PET) is the non-invasive reference standard for myocardial blood flow (MBF) quantification. Hybrid PET-MR allows simultaneous PET and cardiac magnetic resonance (CMR) acquisition under identical experimental and physiological conditions. This study aimed to determine feasibility of simultaneous 13N-Ammonia PET and dynamic contrast-enhanced CMR MBF quantification in phantoms and healthy volunteers.
Methods
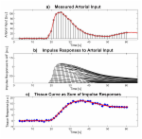
Images were acquired using a 3T hybrid PET-MR scanner. Phantom study: MBF was simulated at different physiological perfusion rates and a protocol for simultaneous PET-MR perfusion imaging was developed. Volunteer study: five healthy volunteers underwent adenosine stress. 13N-Ammonia and gadolinium were administered simultaneously. PET list mode data was reconstructed using ordered subset expectation maximisation. CMR MBF was quantified using Fermi function-constrained deconvolution of arterial input function and myocardial signal. PET MBF was obtained using a one-tissue compartment model and image-derived input function.
Results
Phantom study: PET and CMR MBF measurements demonstrated high repeatability with intraclass coefficients 0.98 and 0.99, respectively. There was high correlation between PET and CMR MBF ( r = 0.98, p < 0.001) and good agreement (bias − 0.85 mL/g/min; 95% limits of agreement 0.29 to − 1.98). Volunteer study: Mean global stress MBF for CMR and PET were 2.58 ± 0.11 and 2.60 ± 0.47 mL/g/min respectively. On a per territory basis, there was moderate correlation ( r = 0.63, p = 0.03) and agreement (bias − 0.34 mL/g/min; 95% limits of agreement 0.49 to − 1.18).
Related collections
Most cited references32
- Record: found
- Abstract: found
- Article: found
Quantification of myocardial perfusion by cardiovascular magnetic resonance


- Record: found
- Abstract: found
- Article: found