- Record: found
- Abstract: found
- Article: found
Time to diagnosis of idiopathic pulmonary fibrosis in the IPF-PRO Registry

Read this article at
Abstract
Background
Idiopathic pulmonary fibrosis (IPF) is a progressive disease with high mortality. Patient characteristics associated with diagnostic delays are not well described.
Methods
Subjects who had not been diagnosed with IPF prior to referral and received a new diagnosis of IPF at an enrolling centre for the IPF-PRO ( Idiopathic Pulmonary Fibrosis Prospective Outcomes) Registry were characterised as having a longer (>1 year) or shorter (≤1 year) time from symptom onset to diagnosis and from first imaging evidence of fibrosis to diagnosis. Patient characteristics, evaluations and time to death or lung transplant were compared between these cohorts.
Results
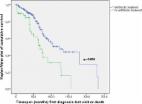
Among 347 patients with a symptom onset date, 49% were diagnosed with IPF >1 year after symptom onset. These patients were slightly younger and had more cardiac comorbidities than patients diagnosed ≤1 year after symptom onset. Among 454 patients with a date for imaging evidence of fibrosis, 78% were diagnosed with IPF ≤1 year later. A greater proportion of patients with >1 year versus ≤1 year from imaging evidence of fibrosis to diagnosis had cardiac comorbidities and gastro-oesophageal reflux. There was no significant difference in time to death or lung transplant between groups by time to diagnosis.
Conclusions
The time from symptom onset to diagnosis remains over 1 year in approximately half of the patients with IPF, but once imaging evidence is obtained, most of the patients are diagnosed within a year. Cardiac conditions and gastro-oesophageal disorders were more commonly reported in patients with a longer time to diagnosis.
Related collections
Most cited references20
- Record: found
- Abstract: found
- Article: not found
Diagnostic criteria for idiopathic pulmonary fibrosis: a Fleischner Society White Paper
- Record: found
- Abstract: found
- Article: found
The European IPF registry (eurIPFreg): baseline characteristics and survival of patients with idiopathic pulmonary fibrosis
- Record: found
- Abstract: found
- Article: not found