- Record: found
- Abstract: not found
- Article: not found
Successful management of intracranial hemorrhage in patient with COVID-19 vaccine-induced immune thrombotic thrombocytopenia and cerebral venous thrombosis: A case report
letter
Read this article at

There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
To the editor,
The COVID-19 vaccine has become widely available worldwide due to the 2019 Coronavirus
disease (COVID-19) pandemic. AstraZeneca's COVID-19 (ChAdOx1) vaccine has been known
to cause vaccine-induced immune thrombotic thrombocytopenia (VITT), which is a medical
term used to describe the development of low platelet counts following vaccination.
In this paper, a case of a Taiwanese man with VITT-induced cerebral venous sinus thrombosis
(CVST) was presented.
1
Through a multidisciplinary approach, that is, intravenous immune globulin (IVIG),
anticoagulant therapy, plasmapheresis, and a minimally invasive surgical technique
by mini-pterional (MPT) craniotomy,
2
we successfully treated this case.
This 41-year-old Taiwanese man came to our institute with progressive headache and
conscious disturbance. He received his first dose of the COVID-19 AstraZeneca vaccine
10 days prior to admission. A brain MR (magnetic resonance) angiography with venography
showed right temporal intra-parenchymal hemorrhage, but no evidence of venous thrombosis
(Fig. 1
A–D). The platelet counts of the patient were only 62x 109 (reference range: 150–400
(109/L))
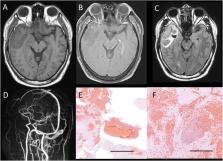
Fig. 1
Magnetic resonance (MR) imaging of patient with vaccine induced cerebral venous thrombosis.
On T1 pre-contrast (A), post-contrast MR image (B) with hypointense signal change
and hyperintensity of T2 FLAIR signal (C) indicated acute hemorrhage accident at right
temporal base area. The Post contrast enhanced MR venography did not detect venous
sinus thrombosis (D). Histopathology indicated (E) multiple hemorrhage lesions, Hematoxylin–eosin
(H&E) stain, scale bar: 2 mm; (F) organization of a thrombus, scale bar: 200μm (H&E).
Fig. 1
The patient underwent a right-side mini-pterional craniotomy to remove the hematoma
after admission due to an ipsilateral dilated pupil from impending brain herniation.
Postoperative computed tomography (CT) scan indicated a new onset of left frontal
hemorrhage which was not life threatening. Due to persistent low platelet count, the
patient received another course of plasmapheresis for 7 days. Systemic corticosteroids
were also subsequently prescribed. The result of anti-platelet factor 4 antibody assessment
was positive, which proved the diagnosis of VITT. The pathology report confirmed the
diagnosis of CVST (Fig. 1E and F). The patient discharged with a good outcome (modified
Rankin Scale = 1).
Several cases of VITT induced CVST after adenoviral vector COVID-19 vaccines have
been reported with a high mortality rate of about 40–50%, which is more significant
than other type of CVST.
1
,
3
The mechanism of VITT is similar to that of heparin-induced thrombocytopenia (HIT).
The mainstream treatments for patients with vaccine induced CVST are high-dose IVIG
with anticoagulation using direct oral anticoagulants (DOAC) or alternative anticoagulants
to heparin including argatroban.
1
Decompressive craniectomy should be considered if there is an occupying cerebral
edema or brain hemorrhage.
4
,
5
In this case, it was believed that early craniotomy for hematoma removal under MPT
craniotomy can achieve equivalent results and can prevent further surgical mobility
by large craniectomy wound in patient with coagulopathy. Though mortality rate of
CVST after COVID-19 vaccination is high, early surgical treatment for intracranial
hemorrhage using minimally invasive surgical techniques, in combination with the best
medical care, may improve clinical outcomes.
Related collections
Most cited references5
- Record: found
- Abstract: found
- Article: found
Ischaemic stroke as a presenting feature of ChAdOx1 nCoV-19 vaccine-induced immune thrombotic thrombocytopaenia
Talal Al-Mayhani, Sadia Saber, Matthew Stubbs … (2021)
- Record: found
- Abstract: not found
- Article: not found
Diagnosis and Management of Cerebral Venous Sinus Thrombosis with Vaccine-Induced Thrombotic Thrombocytopenia
(2021)
- Record: found
- Abstract: found
- Article: not found
The minipterional craniotomy: technical description and anatomic assessment.
Mark C. Preul, Marcelo Crusius, Peter Nakaji … (2007)