- Record: found
- Abstract: found
- Article: found
Une spondylodiscite tuberculeuse chez une transplantée rénale compliquée d’une mycose systémique Translated title: Spinal tuberculosis in renal transplant complicated by systemic fungal infection
Abstract
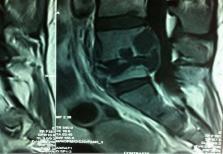
En transplantation, les complications infectieuses sont fréquentes et de diagnostic souvent délicat. Elles peuvent coexister chez le transplanté rénal rendant leur diagnostic encore plus difficile. Le but de ce cas clinique est de discuter les difficultés diagnostiques et de surveillance de deux types de pathologies assez fréquentes chez le transplanté rénal, qui sont la tuberculose et la mycose, à travers l’observation clinique d’une patiente de 24 ans transplantée rénale qui présente une spondylodiscite tuberculeuse et qui développe secondairement une septicémie à Candida non albicans à point de départ urinaire dont le seul point d’appel est la fièvre post opératoire.
Related collections
Most cited references11
- Record: found
- Abstract: found
- Article: not found
Tuberculosis.
- Record: found
- Abstract: found
- Article: not found
Mycobacterium tuberculosis infection in recipients of solid organ transplants.
- Record: found
- Abstract: found
- Article: not found