- Record: found
- Abstract: found
- Article: not found
Retroperitoneal Actinomycosis: A Rare Sequela of an Infected Obstructing Ureteral Stone
Read this article at

Abstract
Background: Actinomycosis is a condition in which Actinomyces, a normal component of the oral and gastrointenstial flora, becomes pathogenic in the setting of damaged tissue, leading to widespread tissue destruction across fascial planes. Prior literature describing this condition is rare, particularly cases involving the retroperitoneum. In this study, we report a case of retroperitoneal actinomycosis caused by an infected, obstructing ureteral stone.
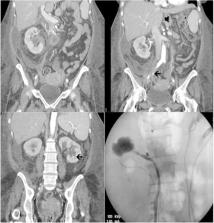
Case Presentation: A 48-year-old woman with a history of substance abuse, malnutrition, and gastric bypass presented to the emergency room with a 3-week history of abdominal pain and fevers. Workup revealed a 9 mm obstructing right ureteral stone with associated perinephric fluid collection that was concerning for forniceal rupture. There was left hydronephrosis and a 3 mm lower pole renal calculus as well. The patient underwent emergent decompression where bilateral duplicated collecting systems were identified, requiring stenting of all four moieties to ensure maximal decompression in the setting of obstructive pyelonephritis. Urine cultures grew Escherichia coli and Candida. The patient continued to deteriorate despite culture appropriate antibiotic therapy; repeat scan revealed progression of her perinephric fluid collection into a loculated retroperitoneal abscess. A percutaneous drain was placed, and nearly half a liter of pus was evacuated. Fluid cultures grew Actinomyces, and she ultimately recovered after a prolonged course of antibiotics, including 1 month of intravenous therapy and an additional 6 months of oral treatment. All stones were ultimately removed via ureteroscopy.
Conclusion: Actinomycosis is a rare invasive infection that is caused when the Actinomyces bacteria colonizes damaged tissue. We present the first reported case of urolithiasis inciting this process via tissue damage caused by obstruction and infection. Although rare, heightened suspicion is warranted among immunocompromised hosts who do not improve after decompression in such scenarios.
Related collections
Most cited references4

- Record: found
- Abstract: found
- Article: found
Actinomycosis: etiology, clinical features, diagnosis, treatment, and management

- Record: found
- Abstract: found
- Article: found
Clinical features of actinomycosis
- Record: found
- Abstract: found
- Article: not found