- Record: found
- Abstract: found
- Article: found
Early hyperoxemia may not increase mortality after cardiac arrest: a pilot study
Read this article at
Abstract
Objective
International Liaison Committee on Resuscitation guidelines advocate an arterial saturation of 94% to 96% after return of spontaneous circulation (ROSC). However, a few clinical trials have investigated the impact of postresuscitative O 2 therapy after cardiac arrest. We studied whether early hyperoxemia is associated with a poor post-ROSC outcome after in-hospital cardiac arrest.
Methods
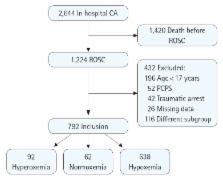
We retrospectively reviewed patients who experienced an in-hospital cardiac arrest from January 2005 to January 2011. Based on the results of the first arterial blood gas analysis (ABGA) within 10 minutes and a second ABGA from 60 to 120 minutes after ROSC, patients were classified into three groups: hyperoxemia (PaO 2 ≥ 300 mmHg), normoxemia (300 mmHg > PaO 2 ≥ 60 mmHg), and hypoxemia (PaO 2 < 60 mmHg or ratio of PaO 2 to fraction of inspired oxygen < 300). We examined whether early hyperoxemia was associated with survival and neurological outcome.
Results
There were 792 patients who met the inclusion criteria: 638 (80.6%) in the hypoxemia group, 62 (7.8%) in the normoxemia group, and 92 (11.6%) in the hyperoxemia group. Multiple logistic regression analysis showed that hyperoxemia was not associated with survival (odds ratio [OR], 1.07; 95% confidence interval [CI], 0.30 to 3.84) or neurological outcome (OR, 1.03; 95% CI, 0.31 to 3.40).
Related collections
Most cited references26
- Record: found
- Abstract: found
- Article: not found
Cardiopulmonary resuscitation with assisted extracorporeal life-support versus conventional cardiopulmonary resuscitation in adults with in-hospital cardiac arrest: an observational study and propensity analysis.
- Record: found
- Abstract: found
- Article: not found
First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults.
- Record: found
- Abstract: found
- Article: not found