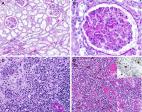
Since late December, 2019, an outbreak of a novel coronavirus disease (COVID-19; previously known as 2019-nCoV)1, 2 was reported in Wuhan, China, 2 which has subsequently affected 26 countries worldwide. In general, COVID-19 is an acute resolved disease but it can also be deadly, with a 2% case fatality rate. Severe disease onset might result in death due to massive alveolar damage and progressive respiratory failure.2, 3 As of Feb 15, about 66 580 cases have been confirmed and over 1524 deaths. However, no pathology has been reported due to barely accessible autopsy or biopsy.2, 3 Here, we investigated the pathological characteristics of a patient who died from severe infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) by postmortem biopsies. This study is in accordance with regulations issued by the National Health Commission of China and the Helsinki Declaration. Our findings will facilitate understanding of the pathogenesis of COVID-19 and improve clinical strategies against the disease. A 50-year-old man was admitted to a fever clinic on Jan 21, 2020, with symptoms of fever, chills, cough, fatigue and shortness of breath. He reported a travel history to Wuhan Jan 8–12, and that he had initial symptoms of mild chills and dry cough on Jan 14 (day 1 of illness) but did not see a doctor and kept working until Jan 21 (figure 1 ). Chest x-ray showed multiple patchy shadows in both lungs (appendix p 2), and a throat swab sample was taken. On Jan 22 (day 9 of illness), the Beijing Centers for Disease Control (CDC) confirmed by reverse real-time PCR assay that the patient had COVID-19. Figure 1 Timeline of disease course according to days from initial presentation of illness and days from hospital admission, from Jan 8–27, 2020 SARS-CoV-2=severe acute respiratory syndrome coronavirus 2. He was immediately admitted to the isolation ward and received supplemental oxygen through a face mask. He was given interferon alfa-2b (5 million units twice daily, atomisation inhalation) and lopinavir plus ritonavir (500 mg twice daily, orally) as antiviral therapy, and moxifloxacin (0·4 g once daily, intravenously) to prevent secondary infection. Given the serious shortness of breath and hypoxaemia, methylprednisolone (80 mg twice daily, intravenously) was administered to attenuate lung inflammation. Laboratory tests results are listed in the appendix (p 4). After receiving medication, his body temperature reduced from 39·0 to 36·4 °C. However, his cough, dyspnoea, and fatigue did not improve. On day 12 of illness, after initial presentation, chest x-ray showed progressive infiltrate and diffuse gridding shadow in both lungs. He refused ventilator support in the intensive care unit repeatedly because he suffered from claustrophobia; therefore, he received high-flow nasal cannula (HFNC) oxygen therapy (60% concentration, flow rate 40 L/min). On day 13 of illness, the patient's symptoms had still not improved, but oxygen saturation remained above 95%. In the afternoon of day 14 of illness, his hypoxaemia and shortness of breath worsened. Despite receiving HFNC oxygen therapy (100% concentration, flow rate 40 L/min), oxygen saturation values decreased to 60%, and the patient had sudden cardiac arrest. He was immediately given invasive ventilation, chest compression, and adrenaline injection. Unfortunately, the rescue was not successful, and he died at 18:31 (Beijing time). Biopsy samples were taken from lung, liver, and heart tissue of the patient. Histological examination showed bilateral diffuse alveolar damage with cellular fibromyxoid exudates (figure 2A, B ). The right lung showed evident desquamation of pneumocytes and hyaline membrane formation, indicating acute respiratory distress syndrome (ARDS; figure 2A). The left lung tissue displayed pulmonary oedema with hyaline membrane formation, suggestive of early-phase ARDS (figure 2B). Interstitial mononuclear inflammatory infiltrates, dominated by lymphocytes, were seen in both lungs. Multinucleated syncytial cells with atypical enlarged pneumocytes characterised by large nuclei, amphophilic granular cytoplasm, and prominent nucleoli were identified in the intra-alveolar spaces, showing viral cytopathic-like changes. No obvious intranuclear or intracytoplasmic viral inclusions were identified. Figure 2 Pathological manifestations of right (A) and left (B) lung tissue, liver tissue (C), and heart tissue (D) in a patient with severe pneumonia caused by SARS-CoV-2 SARS-CoV-2=severe acute respiratory syndrome coronavirus 2. The pathological features of COVID-19 greatly resemble those seen in SARS and Middle Eastern respiratory syndrome (MERS) coronavirus infection.4, 5 In addition, the liver biopsy specimens of the patient with COVID-19 showed moderate microvesicular steatosis and mild lobular and portal activity (figure 2C), indicating the injury could have been caused by either SARS-CoV-2 infection or drug-induced liver injury. There were a few interstitial mononuclear inflammatory infiltrates, but no other substantial damage in the heart tissue (figure 2D). Peripheral blood was prepared for flow cytometric analysis. We found that the counts of peripheral CD4 and CD8 T cells were substantially reduced, while their status was hyperactivated, as evidenced by the high proportions of HLA-DR (CD4 3·47%) and CD38 (CD8 39·4%) double-positive fractions (appendix p 3). Moreover, there was an increased concentration of highly proinflammatory CCR6+ Th17 in CD4 T cells (appendix p 3). Additionally, CD8 T cells were found to harbour high concentrations of cytotoxic granules, in which 31·6% cells were perforin positive, 64·2% cells were granulysin positive, and 30·5% cells were granulysin and perforin double-positive (appendix p 3). Our results imply that overactivation of T cells, manifested by increase of Th17 and high cytotoxicity of CD8 T cells, accounts for, in part, the severe immune injury in this patient. X-ray images showed rapid progression of pneumonia and some differences between the left and right lung. In addition, the liver tissue showed moderate microvesicular steatosis and mild lobular activity, but there was no conclusive evidence to support SARS-CoV-2 infection or drug-induced liver injury as the cause. There were no obvious histological changes seen in heart tissue, suggesting that SARS-CoV-2 infection might not directly impair the heart. Although corticosteroid treatment is not routinely recommended to be used for SARS-CoV-2 pneumonia, 1 according to our pathological findings of pulmonary oedema and hyaline membrane formation, timely and appropriate use of corticosteroids together with ventilator support should be considered for the severe patients to prevent ARDS development. Lymphopenia is a common feature in the patients with COVID-19 and might be a critical factor associated with disease severity and mortality. 3 Our clinical and pathological findings in this severe case of COVID-19 can not only help to identify a cause of death, but also provide new insights into the pathogenesis of SARS-CoV-2-related pneumonia, which might help physicians to formulate a timely therapeutic strategy for similar severe patients and reduce mortality. This online publication has been corrected. The corrected version first appeared at thelancet.com/respiratory on February 25, 2020