- Record: found
- Abstract: found
- Article: found
ROBOTIC TRANS-ABDOMINAL PREPERITONEAL APPROACH (TAPP) APPROACH FOR LATERAL INCISIONAL HERNIAS Translated title: ABORDAGEM ROBÓTICA TRANSABDOMINAL PRÉ-PERITONEAL (RTAPP) PARA HÉRNIAS INCISIONAIS LATERAIS
ABSTRACT
Background:
Lateral incisional hernias arise between the linea alba and the posterior paraspinal muscles. Anatomical boundaries contain various topographic variations, such as multiple nearby bony structures and paucity of aponeurotic tissue that make it particularly challenging to repair.
Methods:
Retrospective data was collected from four patients who underwent robotic-assisted repair of their lumbar hernias after open nephrectomies.
Results:
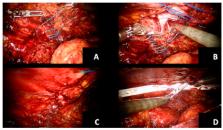
Age ranged from 41-53 y. Two patients had right sided flank hernias while the other two on the left. One patient had a recurrent hernia on the left side. The patients were placed in lateral decubitus position contralateral to the hernia defect side. A trans-abdominal preperitoneal approach was used in all cases. Each case was accomplished with two 8 mm robotic ports, a 12 mm periumbilical port, and a 5 mm assistance port that allowed docking on the ipsilateral hernia side. The hernias were identified, a preperitoneal plane was created, and the hernia sac completely dissected allowing for complete visualization of the defect. All defects were primarily closed. Polypropylene or ProGrip TM mesh was applied with at least 5 cm overlap and secured using either #0 Vicryl ® transfacial sutures, Evicel ® or a combination of both. The peritoneal space was closed with running suture and the ports were removed and closed. The average surgical length was 4 hr. The post-operative length of stay ranged from 0-2 days.
RESUMO
As hérnias incisionais laterais surgem entre a linha alba e os músculos paravertebrais posteriores. Os limites anatômicos contêm várias variações topográficas, como várias estruturas ósseas próximas e escassez de tecido aponeurótico que tornam o reparo particularmente difícil .
Dados foram coletados retrospectivamente de quatro pacientes que foram submetidos ao reparo de hérnia lombar após nefrectomias abertas por técnica robótica. Os pacientes tinham entre 41-53 anos de idade. Dois possuíam hérnia no flanco direito e os outros dois no flanco esquerdo.
Os pacientes foram colocados em posição de decúbito lateral contralateral ao lado do defeito. Abordagem pré-peritoneal transabdominal foi realizada em todos os casos. Cada procedimento foi realizado com dois trocárteres robóticos de 8 mm, um periumbilical de 12 mm e um auxiliar de 5 mm, permitindo docking ipsilateral ao lado da hérnia. As hérnias foram identificadas, plano pré-peritoneal foi criado e o saco herniário completamente dissecado, permitindo completa visualização do defeito. Todos os defeitos foram fechados primariamente com fio de sutura 0/1V-Loc. Tela de polipropileno ou ProGrip TM foi usada com pelo menos 5 cm de overlap e fixada com sutura transfacial com Vicryl ® 0, Evicel ® ou combinação dos dois. O espaço pré-peritoneal foi fechado com sutura contínua e os trocárteres removidos. O tempo operatório médio foi de 4 h. O tempo de permanência hospitalar variou entre 0-2 dias.
Related collections
Most cited references19
- Record: found
- Abstract: found
- Article: not found
Classification of primary and incisional abdominal wall hernias
- Record: found
- Abstract: found
- Article: not found
Controversies in the current management of lumbar hernias.
- Record: found
- Abstract: found
- Article: not found