- Record: found
- Abstract: found
- Article: found
Cost-Effectiveness of Extended and One-Time Screening Versus No Screening for Non-Valvular Atrial Fibrillation in the USA
Read this article at
Abstract
Background
There is limited evidence on the clinical and cost benefits of screening for atrial fibrillation (AF) with electrocardiogram (ECG) in asymptomatic adults.
Methods
We adapted a previously published Markov model to evaluate the clinical and economic impact of one-time screening for non-valvular AF (NVAF) with a single 12-lead ECG and a 14-day extended screening with a hand-held ECG device (Zenicor single-lead ECG, Z14) compared with no screening. Clinical events considered included ischemic stroke, systemic embolism, major bleeds, myocardial infarction, and death. Epidemiology and effectiveness data for extended screening were from the STROKESTOP study. Risks of clinical events in NVAF patients were derived from ARISTOTLE. Analyses were conducted from the perspective of a third-party payer, considering a population with undiagnosed NVAF, aged 75 years in the USA. Costs and utilities were discounted at a 3% annual rate. Parameter uncertainty was formally considered via deterministic and probabilistic sensitivity analyses (DSA and PSA). Structural uncertainty was assessed via scenario analyses.
Results
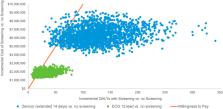
In a hypothetical cohort of 10,000 patients followed over their lifetimes, the number of additional AF diagnoses was 54 with 12-lead ECG and 255 with Z14 compared with no screening. Both screening strategies led to better health outcomes (ischemic strokes avoided: ECG 12-lead, 9.8 and Z14, 42.2; quality-adjusted life-years gained: ECG 12-lead, 31 and Z14, 131). Extended screening and one-time screening were cost effective compared with no screening at a willingness-to-pay (WTP) threshold of $100,000 per QALY gained ($58,728/QALY with ECG 12-lead and $47,949/QALY with Z14 in 2016 US dollars). ICERs remained below $100,000 per QALY in all DSA, most PSA runs, and in all scenario analyses except for a scenario assuming low anticoagulation persistence.
Related collections
Most cited references29
- Record: found
- Abstract: found
- Article: not found
Preference-Based EQ-5D index scores for chronic conditions in the United States.
- Record: found
- Abstract: found
- Article: not found
Screening for Atrial Fibrillation: A Report of the AF-SCREEN International Collaboration.
- Record: found
- Abstract: found
- Article: not found