- Record: found
- Abstract: found
- Article: found
Multifocal bilateral desmoid tumour of perirenal tissues with peribiliary localization
Read this article at
Abstract
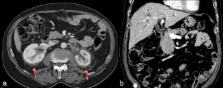
Desmoid tumour (DT) is an unusual, benign tumour, more frequently observed in patients with familial polyposis and pregnant females. It usually presents as a single mass lesion, more frequently showing a compressive rather than an infiltrative growth pattern. We report a case of a 70-year-old male presenting with a multifocal, bilateral infiltrative DT of the perirenal tissue, with involvement of the choledochus wall. The patient was partly treated with tamoxifen and docetaxel, but both therapies were discontinued in accordance with the patient’s decision owing to mild toxicity; however, a CT examination performed 3 months later showed an unexpected remarkable reduction of the tumour at all sites. At 1 year follow-up, new pathologic tissue was visible surrounding the right renal pelvis and the calices.
Related collections
Most cited references9
- Record: found
- Abstract: found
- Article: not found
Desmoid tumors: clinical features and treatment options for advanced disease.
- Record: found
- Abstract: found
- Article: not found
High-dose tamoxifen and sulindac as first-line treatment for desmoid tumors.
- Record: found
- Abstract: found
- Article: not found