
INTRODUCTION
Influenza is an infectious disease that causes harm to human health and inflicts huge economic losses. Influenza mortality rates in different age groups vary from tens to hundreds of cases during epidemics and comprise up to 1,000 cases per 100,000 people during pandemics [1, 2, 3]. The majority of influenza-associated deaths are due to secondary bacterial complications with pneumonia being the major cause. 200 million of the 429.2 million cases of pneumonia reported annually are those that occurred following acute respiratory viral infections (ARVIs) including influenza with 3 to 4 million lethal outcomes (7% of overall mortality) [2, 4]. Approx. 43-67% of pneumonia cases following ARVIs are reported for children under 5 years old putting them at particular risk [5]. The prevalence of pneumonia is shown to increase following influenza epidemics/pandemics. Therefore, a significant increase in the pneumonia mortality rate was recorded during the pandemics of 1918, 1957, 1968, and 2009 [5, 6]. The histological and microbiological examination of autopsy samples taken from individuals who died during the 1918 Spanish influenza pandemic revealed that the majority of the deaths were caused by secondary pneumonia. Streptococcus pneumoniae (S. pneumoniae) and Staphylococcus aureus (S. aureus) are the most common etiological agents at secondary pneumonias. The analysis of clinical data showed that bacterial pneumonias account for 30% of complications following pandemic influenza virus A/California/07/2009 (H1N1)pdm09 infection, with S. aureus being the most frequently reported disease-causing agent [7, 8]. Prevention and proper treatment of influenza infection seem to be the best strategy to reduce secondary complications from influenza. In particular, it was found that influenza vaccination reduces hospital admissions due to pneumonia in elderly individuals and the use of anti-influenza drugs to treat the infection lowers the rate of further bacterial complications [5]. The same effect was shown in an experimental model for the secondary bacterial pneumonia following influenza infection [9-11]. The use of oseltamivir, a neuraminidase inhibitor, in mice infected with influenza A virus and later with S. pneumoniae, reduced the mortality due to secondary bacterial pneumonia developed following the influenza infection, decreased the disease symptoms, and facilitated the course of the infection [12]. Similar results were obtained with fludaza (NeoBix, USA), a drug undergoing phase III clinical trials, and with umifenovir, an anti-influenza drug licensed by Pharmstandard (Russia) [13, 14].
The novel original drug that belongs to the azoloazine class of compounds, triazavirine (an analogue of purine nucleotide guanine), is licensed in Russia [15]. This drug was developed jointly by the scientists of Ural State Polytechnic University (Ekaterinburg, Russia), Postovsky Institute of Organic Synthesis (Ekaterinburg, Russia), and Research Institute of Influenza (St. Petersburg, Russia). Тriazavirine has a broad spectrum of antiviral activity and is effective against a number of acute respiratory virus infections, including influenza A and B. The goal of this project was to study the efficacy of triazavirine against secondary bacterial pneumonia following influenza in mice.
MATERIALS AND METHODS
Compounds
Triazavirine (2-methylthio-6-nitro-1,2,4-triazolo[5,1-c]1,2,4-triazine-7(4I’)-one) was provided by Medsynthesis (Russia) (Fig. 1A) [15].
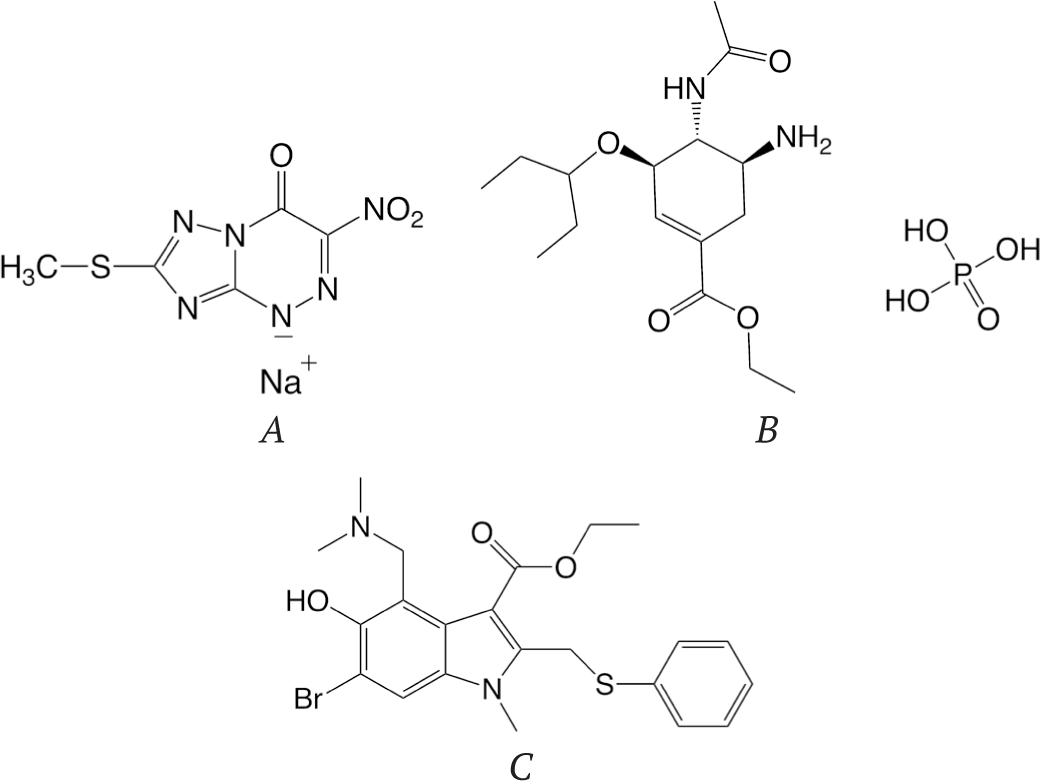
Oseltamivir phosphate (Ethyl (3R,4R,5S)-4-acetamido-5-amino-3-(pentan-3-yloxy)cyclohex-1-ene-1-carboxylate phosphate) (Fig. 1B) was a gift from Chemical Diversity, Inc. (San-Diego, USA). Umifenovir (Ethyl 6-bromo-4-[(dimethylamino)methyl]-5-hydroxy-1-methyl-2-[(phenylthio)methyl)]-1H-indole-3-carboxylate) (Fig. 1C) was provided by Pharmstandard (Russia). Oseltamivir phosphate and triazavirine were dissolved in sterile distilled water. For the oral delivery to mice, umifenovir was suspended in 1% starch solution. For each experiment, the freshly made solutions of drugs were used.
Cells and influenza viruses
Madin Darby canine kidney (MDCK) cells were grown at 37°C in a humidified atmosphere of 5% CO2 in minimal essential medium (MEM) supplemented with 10% fetal bovine serum (FBS), 5 mM L-glutamine, 25 mM HEPES, 100 U/ml penicillin, 100 μg/ml streptomycin sulfate, and 100 μg/ml kanamycin sulfate. Influenza virus A/California/04/2009 (H1N1)pdm09 (A/CA/04/09) was provided by the WHO collaborating Center Research Institute of Influenza (St. Petersburg, Russia). The virus was propagated in embryonated chicken eggs (CE). The virus infectious titer was determined by titration in CE and expressed as a decimal logarithm of embryonated infectious doses (log10EID50/ml). The strain S. aureus 1986 was obtained from the collection of the Mechnikov Institute for Vaccines and Sera (Moscow, Russia). Bacteria were propagated on tryptic soy agar.
Assessment of drug efficacy in mouse models
Female BALB/c mice that were obtained from the Scientific Center of Biomedical Technologies of the Russian Academy of Science (Andreevka, Moscow region, Russia) weighing approximately 12 to 14 g were quarantined and acclimated for 3 days prior to use. Mice were housed in cages and used for treatment in groups of 13 animals. All the studies were approved by the Mechnikov Research Institute of Vaccines and Sera Committee on the Ethics of Animal Experiments and were conducted in strict accordance with the applicable laws and guidelines.
For animal infection mouse-adapted A/CA/04/09 virus was obtained by 3 subsequent passages in mouse lungs. In order to study the efficacy of drugs against influenza infection mice were intranasally (i.n.) challenged with mouse lethal dose (MLD80/0.1 ml), which is equal to 4.0 log10EID50/0.1 ml) of A/CA/04/09 virus. In the experiments dealing with secondary bacterial pneumonia following influenza, the animals were infected i.n. with 0.5 MLD50/0.1 ml of mouse-adapted A/CA/04/09 virus. S. aureus stocks were grown overnight in tryptic soy broth at 37°C and diluted in sterile PBS to 2x1010 of colony forming units (CFU/0.1 ml) prior to use. S. aureus challenge was performed i.n. on day 4 after the virus infection. Prior to the intranasal delivery of infectious agents, the animals were lightly anesthetized by ether.
In all our experiments, antivirals were administered to mice intragastrically (i.g.) by oral gavage in the volume of 200 μl. Triazavirine was administered for 5 consecutive days starting from 24 h before the viral inoculation in the dose of 25, 50, or 100 mg/kg/day of mouse body weight twice a day. Umifenovir served as a positive control and was administered for 5 consecutive days starting 24 h before viral inoculation in the dose of 60 mg/kg/day once per day (in the morning). Oseltamivir was used as a second positive control and was administered 6 h before viral inoculation in the dose of 10 mg/kg/day and for 5 consecutive days twice a day. Animals of the placebo group were treated by PBS. From day 0 to day 15 post infection (p.i.), the animals were weighed and the weight loss/gain was calculated for each mouse as a percentage of body weight to day 0 before the virus inoculation. The reported values are expressed as mean value ± standard deviation (SD). Animals that showed signs of severe disease and weight loss of ≥ 25% were humanely euthanized. The survival rate of the animals was monitored for 21 days. The efficacy of the corresponding antiviral agent was determined according to the number of mice that survived 21 days post infection, the mean number of days to death, and weight loss. The mean survival day (MSD) was calculated by the formula: MSD=[f(d-1)]/n, where f is the number of the mice that survived at day d, and n is the total number of mice in the group.
Lung examination
3 mice from each group were euthanized at the 4th or 7th day post-viral infection from the groups infected only with virus and with both the virus and bacteria, respectively. The viral titers and bacterial counts were estimated in the lungs. The lung homogenates were prepared, spun at 10 g for 5 min, and the supernatants were used for the determination of virus titers and/or bacterial counts. Quantification of the S. aureus colonies was done in tenfold dilutions of lung supernatant added to tryptic soy agar plates supplemented with 3% sheep erythrocytes (vol/vol). Identification of the colonies was done by visual inspection. Virus titers were determined by the titration of lung homogenates on MDCK cell monolayers and expressed as a decimal logarithm of the tissue culture infectious doses (log10TCID50/ml).
RESULTS
Efficacy of triazavirine in mice infected with influenza virus
As it was shown earlier [16], without prior adaptation influenza virus A/CA/04/09 does not kill mice but causes a transient weight reduction (up to 11%). Therefore, the virus A/CA/04/09 was first adapted to mice by consecutive passages in the mouse lungs, and then was used in experiments to estimate the efficacy of the antivirals. In the first set of experiments, we studied the efficacy of triazavirine in mice infected with the MLD80 of mouse-adapted A/CA/04/09 virus. Two antiviral drugs with a different mechanism of action – neuraminidase inhibitor oseltamivir and fusion inhibitor umifenovir – were used as the controls. A high mortality rate (80%) and loss of body weight (10%) were observed after the viral infection in the control group of mice that were placebo treated (PBS) (Fig. 2 A, B). Of the three triazavirine dose regimens (25, 50, and 100 mg/kg/day), only the first one significantly enhanced the survival of animals (60% vs. 20%, p <0.05) in comparison to the placebo control group (Fig. 2A). Administration of triazavirine at 25 mg/kg/day also resulted in the enhancement of the mean survival time to 12.8 days compared to 10 days for the placebo treated control group of mice. Triazavirine at dose of 50 mg/kg/day provided the survival rate of 45%, which was not significantly different from that of the placebo control group. The survival rate and a mean survival time for the group of mice treated with 100 mg/kg/day of triazavirine did not differ from that of the mice in the control group. The animals in all the infected mouse groups after the treatment demonstrated weight loss as well as mice in the placebo treated group. However, in the group of animals that was treated with triazavirine at 25 mg/kg/day the increase of body weight observed starting from day 7 p.i. (Fig. 2B).

The most profound therapeutic effect was observed for oseltamivir at 10 mg/kg/day and umifenovir at 60 mg/kg/day. The administration of these antivirals completely protected the infected mice from death and prevented their weight loss (Fig. 2A, B).
The virus titers in the lungs of mice were measured at day 4 p.i. and are shown in Fig. 3. The corresponding virus titers for animals from the group treated with triazavirine at dose 25 mg/kg/day were significantly lower compared to those for the placebo control group (2.8±1.0 vs 5.2±0.6, p < 0.05, respectively). Treatment of mice with triazavirine at doses of 50 and 100 mg/kg/day, as well as with umifenovir and oseltamivir did not result in statistically signifucant reduction of viral titers in lungs (Fig. 3).

Efficacy of triazavirine in the model of secondary bacterial pneumonia following influenza infection
In the next set of experiments, we studied the effect of triazavirine treatment on mice that were first infected with influenza virus and 4 days later challenged with S. aureus. In these experiments, we infected the animals with a sublethal dose 0.5 MLD50 of the mouse-adapted influenza virus A/CA/04/09 or mock-infected them with PBS and 4 days later challenged the same groups of mice with 2x1010 CFU of S. aureus. The virus infection at this dose did not cause the death of animals in the virus control group (infected with the virus only). In the bacterial control group (exposed to intranasal infection with S. aureus only), no deaths were reported as well. All mice infected with the virus followed by the infection with bacteria died in 11/7 days after the virus/bacterial challenge, respectively (Fig. 4A). The combined infection with both pathogens also resulted in significant weight loss (almost 30% on study day 9) (Fig. 4B). The obtained data were confirmed by lung examination. Bacterial co-infection with S. aureus of virus infected mice led to significantly increased viral lung titers (Table). The bacterial densities in the lungs of mice pre-infected with influenza virus were not significantly different compared to the mockinfected mice (Table).

| Treatment | MSD | Virus titer in the lungs at day 4 p.i., log10 TCID50 /mla | Bacterial density in the lungs, CFU/mla |
|---|---|---|---|
| 1. A/CA/04/09 + S. aureus + triazavirine 25 mg/kg/day | 11.4 | 6.5±0.5 | (5.3±1.4) ×105 |
| 2. A/CA/04/09 + S. aureus + triazavirine 50 mg/kg/day | 17.0 | 4.3±0.3* | (3.5±2.5) ×105 |
| 3. A/CA/04/09 + S. aureus + triazavirine 100 mg/kg/day | 16.1 | 3.5±0.5* | (4.0±1.0) ×105 |
| 4. A/CA/04/09 + S. aureus + oseltamivir 10 mg/kg/day | 13.3 | 5.5±0.5 | (2.5±0.8) ×103† |
| 5. A/CA/04/09 + S. aureus + umifenovir 60 mg/kg/day | 16.3 | 5.5±0.5 | (5.2±2.8)×105 |
| 6. A/CA/04/09 + S. aureus | 8.6 | 6.5±0.5 † | (5.6±2.3) ×105 |
| 7. A/CA/04/09 | >21 | 2.5±1.0 | - |
| 8. S. aureus | >21 | - | (4.3±0.6) ×105 |
The data are given as M ± SD.
The difference is significant when compared to the group infected with the virus A/CA/04/09 alone, Student’s t-test, p < 0.001.
The difference is significant when compared to the group of virus infected mice and co-infected with S. aureus, Student’s t-test, p < 0.001.
Triazavirine showed the dose dependent efficacy in the treatment of mice with the secondary bacterial pneumonia following influenza infection. The administration of this drug at 25 mg/kg/day gave a poor effect on the survival rate (25%) and weight loss, but increased the mean survival time. The density of bacteria and the virus titer in animals treated with triazavirine at this low dose did not significantly differ from that in the placebo control group of animals (Table). The administration of triazavirine to mice in doses of 50 and 100 mg/kg/day was more effective. This treatment resulted in significantly enhanced survival of 67-75% of the animals (p<0.001) and increased the time to death by more than twofold, compared to the virus infected mice co-infected with S. aureus (Fig.4 A). These results correlate to the outcome of the lung examination experiments. The administration of triazavirine at 50 and 100 mg/kg/day significantly reduced the virus titer by 2.2 and 3.0 log10TCID50/ml respectively in the treated animals (p < 0.001). No significant reduction of the bacterial counts in the lungs of the animals coinfected with mouse-adapted A/CA/04/09 and S. aureus was noticed (Table). Similar results were observed in the group treated by umifenovir at 60 mg/kg/day, which protected 67% of the mice (p < 0.001) and increased the time to death up to 16.3 days. However, umifenovir did not reduce significantly the virus titer and the density of the bacteria in the lungs of infected animals. The treatment with another antiviral drug, oseltamivir at 10 mg/kg/day, of animals infected with influenza A/CA/04/09 virus followed by infection with S. aureus protected 42% of the animals against death (p < 0.05), and increased the time to death by 1.5 times on average (Fig. 4. A, B). At the same time, the treatment with oseltamivir did not decrease the virus titer, but significantly reduced the density of the bacteria in mouse lungs (p < 0.001, Table).
DISCUSSION
Pneumonia often occurs as a complication after the influenza infection and accounts for a large proportion of the morbidity and mortality associated with seasonal and pandemic influenza outbreaks [5, 7]. Antibiotic therapy alone may not be the most efficacious treatment for this dual infection. However, antiviral therapy has often been ignored because viral infections are usually resolved by the time the bacterial pneumonia occurs. It was shown previously that antiviral treatment with oseltamivir and umifenovir improves the outcome of the secondary bacterial pneumonia after influenza in the mouse model [12-14]. Clinical trials have also confirmed this effect and showed that the antiviral treatment of influenza reduces the risk of post influenza complications [16].
In the present study, the antiviral compound triazavirine was tested in a mouse model of secondary bacterial pneumonia after influenza compared to the mouse model of influenza pneumonia. Treatment with triazavirine in the mouse lethal model of influenza was not highly effective and only at the lowest dose 25 mg/kg/day led to a statistically significant improvement of the animals’ survival rate and extension of mean survival time. The administration of triazavirine at this dose also prevented weight loss in the infected animals. Efficacy of triazavirine treatment decreased with the increase of the drug dose and at 100 mg/kg/day – the highest of the studied doses – triazavirine was not effective at all in this model.
The efficacy of triazavirine treatment in a mouse model of secondary bacterial pneumonia after influenza was more effective and increased along with increasing the drug dose. The administration of triazavirine at the doses 50 and 100 mg/kg/day in our experiments significantly decreased the virus titer and increased the survival post the secondary bacterial pneumonia following influenza in mice. The effectiveness of triazavirine was not inferior to licensed drugs oseltamivir and umifenovir. One of the possible explanations of the significant difference observed in experiments with these two models could be the narrow therapeutic window in infected mice in the first model. Clinical trials showed that triazavirine is well tolerated and safe in humans. Experimental studies revealed that triazavirine has low toxicity in animals including mice (unpublished data). However, it is known that the toxicity of some drugs is significantly higher in infected versus intact animals. Since, in the lethal model, the influenza pneumonia is acute and fast-paced, the therapeutic effect of the drug at high doses could be masked due to the drug toxicity. That effect could be the reason for a contradictory outcome of the experiments using this drug in two different models. For simulation of the secondary bacterial pneumonia after influenza in mice we used the sublethal dose of virus. In that case, the viral infection develops slowly and is less harmful for the infected animals and that makes the effect of the drug more pronounced.
The difference observed in the experiments with triazavirine in two models could also be explained by the mechanism of action of this drug. As it was shown previously [15], triazavirine, being a guanine analogue, is a selective inhibitor of influenza RNA polymerase complexes. In addition, there are some data about its pleiotropic mechanism of action. It was shown that triazavirine affects the formation of amyloid-like fibrils of the model peptide (SI), which determines the pathogenesis of conformational diseases [17]. Moreover, amyloid-like oligomers can also act as signal transducers in healthy and infected organisms [18].
The influenza-bacterial co-infection is a multifactorial process that involves various pathogenic factors of virus and bacteria as well as host responses. All of these factors should be taken into account when considering the incidence and pathogenicity of these co-infections. Experiments in animal models have improved our understanding of how influenza viruses interact with their bacterial co-pathogens and of the accompanying host immune response. The results of these experiments showed that aberrant immune response leads to severe inflammation, a key driver of bacterial acquisition and infection severity following influenza [5, 11].
Therefore, the use of antivirals like triazavirine, which suppress virus replication and significantly increase the survival of animals with a combined virus – bacterial infection could decrease the severity of a secondary bacterial infection of the host organism, and it could be a new method to prevent and treat influenza-associated bacterial co-infections. Further studies are necessary to confirm this effect in humans.