- Record: found
- Abstract: found
- Article: found
Clinical surveillance of the influenza A(H1N1)2009 pandemic through the network of sentinel general practitioners
research-article
20 August 2010
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Introduction
Since the 1950s, sentinel surveillance networks with general practitioners (GPs) have
been progressively implemented and involved in influenza surveillance, e.g. in the
UK, the Netherlands, Belgium, France, Portugal and Spain. Since 1988, several collaborative
European studies with sentinel networks aimed at stimulating influenza surveillance
all over Europe and harmonising the surveillance activities [1-3]. In Belgium, a sentinel
network specifically dedicated to influenza surveillance, with the participation of
about 40 GPs, was initiated in 1985 [4,5] and has participated in various European
influenza related projects. Since autumn 2007, this network is integrated into the
network of the Sentinel General Practitioners (SGPs) existing since 1979 and responsible
for the surveillance of many other health problems [6-8]. Since then, the SGPs have
been continuously involved in the clinical and virological influenza surveillance
[9]. As the SGPs network is not appropriate for the detection of sporadic cases, during
the containment phase of the A(H1N1)2009 (from week 14 till week 28), a comprehensive
surveillance of all suspected cases of A(H1N1)2009 virus among travellers returning
from the USA, Mexico or other countries at risk, was carried out by all Belgian physicians.
As of week 29, the start of the mitigation phase, the SGPs were the most important
tool for the clinical as well as the virological influenza surveillance. The latter
was reinforced with the purpose of following up the A(H1N1)2009 virus circulation
in the general population [10].
The main purposes of this influenza surveillance are the early detection of an influenza
epi-demic, the study of the intensity and duration of the epidemic and the identification
of the circulating viruses. The virological surveillance component is outlined elsewhere
in this issue [10]. This article details the clinical surveillance activities of the
SGPs from week 14, at the appearance of the A(H1N1)2009 virus, until week 53 of 2009.
Method
The SGPs are a nationwide sentinel surveillance network of about 160 voluntarily participating
GPs homogeneously spread over the country. They are as representative as possible
of all GPs in Belgium [11]. Besides the number of acute respiratory infections by
age group, the GPs reported weekly, on a standardised paper form, every patient with
an influenza-like illness (ILI). The general criteria for ILI were: sudden onset of
symptoms, high fever, respiratory (i.e. cough, sore throat) and systemic symptoms
(headache, muscular pain). For every patient, age group (< 5, 5-14, 15-64, 65-84,
85+), hospitalisation, antiviral treatment (as of week 35), delivery of absence from
work certificate, and seasonal and pandemic vaccination status (as of week 42) were
recorded.
Reported ILIs were analysed on a weekly basis for inclusion in the "Weekly Epidemiological
Report Influenza" [12]. This included the weekly reported incidence of ILI for the
whole country, the three regions and separate age groups, as well as the weekly reported
incidence of ILI-related hospitalisations, of ILI patients who have had antiviral
treatment or have been vaccinated for seasonal flu for separate age groups and of
ILI patients for whom work certificates were provided. The estimated number of A(H1N1)2009
related cases in the general population was also included in the weekly report. The
latter was derived from the percentage of A(H1N1)2009-positive ILI cases. Data management,
statistical analysis and reporting were carried out by the Scientific Institute of
Public Health (WIV-ISP), using STATA Version 10 and LaTeX Project software.
Data on vaccination status and work certificates are not presented in this article.
For practical reasons, the data of week 52 and week 53 were analysed together.
Since no patient lists per GP exist in Belgium, the average population coverage per
GP was estimated on the basis of the total Belgian population, divided by the total
number of practising GPs in the country. The latter was based on figures from the
National Institute of Sickness and Invalidity Insurance (NISII) [11]. Thus, the average
population coverage per GP was estimated at 953 inhabitants per GP. The weekly global
population coverage was derived from the total number of participating GPs multiplied
by 953. The age distribution of this estimated population was assumed to be similar
to the national population.
A baseline threshold was calculated using the Moving Epidemics Method (MEM) proposed
by the European Influenza Surveillance Scheme (EISS) baseline working group [13].
In principle, each influenza season is mathematically divided into a pre-epidemic,
epidemic and a post-epidemic period. The proposed baseline threshold is then calculated,
i.e. the upper 95% confidence limit of the geometric mean of the peak pre-epidemic
values. The baseline threshold calculation was based on 5 peak values per influenza
season, in 9 historical seasons 2000/01-2008/09. The baseline threshold is a conservative
value that demarcates the start of the influenza epidemic. When the weekly incidence
rate drops below the post-epidemic baseline, the epidemic period is considered to
have come to an end. For practical purposes, the pre- and post-epidemic baseline values
were considered the same. Based on this model and using two-sided tests, the baseline
threshold was estimated at 141.37 ILI patients seen in general practice per 100,000
inhabitants per week.
In the framework of this surveillance, the criteria used to define the epidemic influenza
period were: weekly incidence rate of ILI patients seen in general practice above
the baseline threshold; > 20% positive specimens among nasopharyngeal swabs taken
in ILI patients; and signs of influenza activity in neighbouring countries.
Results
In the period from week 14 until week 53, between 111 and 162 GPs participated in
the weekly clinical influenza surveillance. The weekly incidence of ILI patients seen
in general practice per 100,000 inhabitants exceeded the baseline threshold for the
first time in week 40 (beginning of October 2009) with an incidence of 173/100,000
inhabitants (95% CI: 152-196). The incidence rate remained above the baseline threshold
until week 49 (at the beginning of December). According to the above-mentioned criteria
the influenza epidemic period lasted 10 weeks, from the beginning of October until
the beginning of December. The epidemic peaked in week 44, with an incidence of 769/100,000
inhabitants (95%CI: 725-815). This peak value is significantly lower (p < 0.05) than
the A(H3N2) seasonal peak in week 4 of 2009 (844/100,000 inhabitants (95%CI: 808-880).
The peak value in week 44 coincided with a peak in the percentage of A(H1N1)2009 virus-positive
swabs [10]. Based on this percentage the extrapolated number of A(H1N1)2009 cases
in the general population in week 44 was estimated at 46,848 (95% CI:43,331-50,641).
Figure 1
Sentinel General Practitioners, incidence of ILI patients in general practice, 2009.
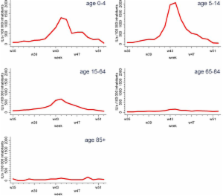
In the course of this epidemic period, the most affected age group was the 5-14-year
olds, followed by the < 5-year olds. People aged 65 years and above were considerably
less affected.
Figure 2
Sentinel General Practitioners, incidence of ILI patients in general practice by age
group, 2009.
In the course of the epidemic period between week 40 and 49, the weekly hospitalisation
rate for ILI patients seen in general practice fluctuated between 0 and 2%.
The weekly percentage of ILI patients with antiviral treatment, recorded as of week
35, varied between 1 and 13%.
Discussion
The network of SGPs has proven to be an important source of information in the influenza
surveillance of the A(H1N1)2009. The SGPs provided information on the start, the duration
and the peak of the epidemic period. Most of the affected persons were children aged
< 15 years. Few ILI patients seen in general practice were hospitalised or got antiviral
treatment.
Table 1
Sentinel General Practitioners, ILI patients with antiviral treatment by age group,
2009
Week
0-4
5-14
15-64
65-84
85+
tot
#
#t
%
#
#t
%
#
#t
%
#
#t
%
#
#t
%
#
#t
%
2009w35
6
0
0
11
0
0
71
1
1
5
0
0
2
0
0
95
1
1
2009w36
7
0
0
12
1
8
84
10
12
4
1
25
0
0
107
12
11
2009w37
12
1
8
22
0
0
115
6
5
10
1
10
0
0
159
8
5
2009w38
10
1
10
31
2
6
120
7
6
9
1
11
2
0
0
172
11
6
2009w39
15
1
7
39
0
0
159
8
5
13
2
15
1
0
0
227
11
5
2009w40
16
0
0
38
0
0
188
9
5
11
2
18
1
0
0
254
11
4
2009w41
21
3
14
67
1
1
238
19
8
13
3
23
1
0
0
340
26
8
2009w42
45
8
18
151
5
3
340
22
6
20
2
10
2
0
0
558
37
7
2009w43
67
5
7
328
27
8
573
61
11
32
4
13
2
0
0
1002
97
10
2009w44
107
8
7
346
9
3
637
39
6
35
3
9
3
0
0
1128
59
5
2009w45
97
4
4
202
5
2
456
26
6
22
4
18
2
1
50
779
40
5
2009w46
40
5
13
116
4
3
348
18
5
20
3
15
1
0
0
525
30
6
2009w47
44
6
14
82
3
4
265
11
4
12
0
0
1
0
0
405
20
5
2009w48
46
0
0
76
3
4
191
9
5
18
5
28
1
0
0
332
17
5
2009w49
26
2
8
46
1
2
127
4
3
15
1
7
4
0
0
219
8
4
2009w50
17
2
12
38
0
0
122
6
5
13
1
8
1
0
0
191
9
5
2009w51
19
4
21
9
1
11
85
11
13
9
0
0
2
0
0
124
16
13
2009w52
6
0
0
10
0
0
89
2
2
31
2
6
2
0
0
138
4
3
# = number of ILIs reported; #t = number of ILI patients treated with antivirals reported;
% = percentage of ILI patients treated with antivirals (#/100 ILIs)
Strengths of the SGPs' influenza surveillance
The SGPs have a long experience in public health surveillance. The highly motivated
partici-pating GPs are a guarantee for the quality of the participation and of the
recorded data. The clinical influenza surveillance data are corroborated by the virological
data originating from the same patients [10]. The continuous weekly influenza monitoring
year after year enables to respond to the influenza surveillance purposes previously
outlined and to compare consecutive influenza seasons as to the intensity and duration
of the epidemics and the type of circulating viruses.
Weaknesses
One weakness is the denominator problem caused by the absence of patient lists per
GP. Only a crude estimation of the denominator population can be made. Further, sensitivity
or completeness of the ILI recording is hampered by the fact that the surveillance
only concerns patients visiting the GP and does not include ILI patients visiting
other health care providers or not consulting at all. Both weaknesses, however, do
not hamper studying the trend in ILI incidence. Finally, the weekly reporting frequency
hinders the daily follow-up of the situation, desirable in an epidemic period.
This does not refrain the SGPs from playing a crucial role in the clinical as well
as in the virological influenza surveillance in this A(H1N1)2009 pandemic.
Related collections
Most cited references6

- Record: found
- Abstract: found
- Article: not found
Tool for validation of the network of sentinel general practitioners in the Belgian health care system.
M P Lobet, Guy Cornelis, G Masuy-Stroobant … (1987)
- Record: found
- Abstract: found
- Article: not found
Five years of sentinel surveillance of acute respiratory infections (1985-1990): the benefits of an influenza early warning system.
A Stroobant, Guy Cornelis, J Lion-Cachet … (1992)