- Record: found
- Abstract: found
- Article: found
ANCA-associated Vasculitis in a Case of Congenital Leptin Deficiency
letter
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Sir,
Leptin (Greek “leptos” = “thin”) is a hormone that helps to regulate metabolism by
inhibiting food intake and promoting energy expenditure. In addition to being a key
factor in regulating body weight, leptin plays an important role in the regulation
of immune system and various other physiological responses.[1] Congenital leptin deficiency,
caused by LEP gene mutation and inherited as an autosomal recessive disorder, presents
with severe obesity early in life, following a normal birth weight. Affected individuals
suffer from hypogonadotropic-hypogonadism, which if untreated leads to delayed puberty
and infertility. This form of leptin deficiency is extremely rare with less than 30
patients reported in the literature so far.[2] Leptin deficiency is also suspected
to be involved in the pathophysiology of ANCA-associated vasculitis (AAV). Kümpers
et al. found that leptin levels are negatively correlated with the disease activity.[3]
Further studies are needed to gauge the role of leptin as a potential therapeutic
target in the treatment of autoimmune disorders.
A 10-year-old girl, a product of second degree consanguineous marriage, first in birth
order, presented with multiple painful, red, raised lesions on the trunk and extremities
since 5 days. Examination revealed palpable purpura and ulcerations of variable sizes
and shapes over the legs, arms, forearms, dorsa of hands and feet, chest, and abdomen
[Figures 1 and 2]. There was predominant extensor distribution with koebnerization
appreciated at places. Mucosae were not involved. General physical examination revealed
moon facies [Figure 3], morbid obesity with a weight of 90 kg, height 137 cm, and
a BMI of 47.95. She had difficulty in walking due to excessive weight. Acanthosis
nigricans was also noted in the axilla and neck [Figure 4]. Rest of the systemic examination
was within normal limits. Investigations revealed neutrophilic leukocytosis (white
blood cell count –19,950/cumm; N = 80.5, L = 17, M = 5.9, E = 01). Liver and renal
parameters, routine and 24 h urinary examination were unremarkable. Rheumatoid factor,
hepatitis B surface antigen, anti-HCV antibodies, HIV ELISA, antinuclear antibody,
lupus anticoagulant, and cryoglobulins were also negative. Fasting plasma glucose
and insulin levels were normal. Triglycerides were marginally raised. cANCA was positive,
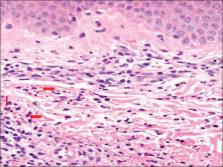
and skin biopsy was suggestive of leukocytoclastic vasculitis with neutrophilic infiltrate
and nuclear debris around vessel walls [Figure 5].
Figure 1
Palpable purpura and ulcerations over the lower limbs
Figure 2
Vasculitic lesions over the abdomen and chest
Figure 3
Moon facies in the affected girl
Figure 4
Acanthosis nigricans on the neck and axilla
Figure 5
Leukocytoclastic vasculitis with neutrophilic infiltrate and nuclear debris (arrows)
(H and E, ×400)
According to her parents, the patient had uneventful antenatal and perinatal period
and was apparently normal till the age of 6 months when they suspected excessive eating
and weight gain by the child. The consultation was sought for the same, and the child
was evaluated for leptin deficiency in view of the early onset obesity. Her anthropometric
measurements at that time were: weight 10.75 kg (>95th percentile), height 64.4 cm
(between 25th and 50th percentile), and BMI 25.84 kg/m2. Baseline investigations,
echocardiography, serum cortisol level, and thyroid function test did not reveal any
abnormality. Serum leptin levels were inappropriately low 0.8 ng/ml (1.7–10.9 ng/ml).
The patient was diagnosed as a case of leptin deficiency but was subsequently lost
to follow-up till date when the patient reported to us with the purpuric rash. During
the intervening period, the patient had normal developmental milestones with no mental
retardation or language deficit.
There was also history of excessive weight gain in her younger 9-month-old male sibling
[Figure 6]. He likewise was of normal weight at birth but was presently obese. His
weight was 9 kg (>90th centile), length was 64 cm (10th centile), and BMI was 21.97
kg/m2. On evaluation, he too was diagnosed as having leptin deficiency (Serum leptin
levels: 1.1 ng/ml). Due to unavailability at our center, genetic analysis could not
be performed in either of the two cases.
Figure 6
Morbid obesity in the younger sibling
The index case was treated with tapering doses of steroids and showed remarkable improvement
of skin lesions. Endocrinology consultation was sought. She was advised leptin replacement
therapy which could not be administered, as the patient could not afford the same.
Congenital leptin deficiency is one of the rare causes of early-onset obesity. It
was first described in two cousins from an inbred Pakistani kindred by Montague et
al.[4] Subsequent cases were reported by Farooqi et al., Gibson et al., Strobel et
al. and Wabitsch et al.[5
6
7
8] A homozygous frameshift or missense mutation in the LEP gene (7q31.3) results in
the characteristic phenotype of severe hyperphagia and extreme obesity early in infancy.
Administration of recombinant human leptin [recombinant methionyl human leptin (r-metHuLeptin)]
has resulted in sustained positive results in this non-syndromic disorder of excessive
weight gain. Active ANCA-associated vasculitis is associated with functionally defective
regulatory T cells and consequently decreased levels of leptin. Kümpers et al. suggested
that low levels of leptin may enhance the inflammatory process in disorders that involve
innate immunity. Invasion and destruction of activated endothelium by primed neutrophils
is a salient feature of vasculitis. Notably, leptin may partake in this process because
microvascular endothelial cells and neutrophils both express the leptin receptor.
It is thus conceivable that leptin attenuates the neutrophil chemotaxis in vasculitis.
Further effects of leptin on microvascular endothelial cells include increased proliferation
and inhibition of apoptosis. However, on the contrary, Yilmaz et al. have shown that
Leptin level was higher in Takayasu arteritis patients than in healthy controls albeit
the difference was not statistically significant.[9] Similarly, studies performed
in other forms of systemic vasculitis (Henoch-Schönlein purpura and Behcet's disease)
have shown increased levels of leptin during active disease periods.[10
11] Whether leptin has a role in vasculitis or its altered levels in this disorder
is a mere coincidental finding needs to be probed. Larger studies are required to
consolidate this finding. Our case emphasizes the need for early detection of congenital
leptin deficiency, which if misdiagnosed runs the risk of severe obesity-associated
complications (especially type II diabetes).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
In the form the patient(s) has/have given his/her/their consent for his/her/their
images and other clinical information to be reported in the journal. The patients
understand that their names and initials will not be published and due efforts will
be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Related collections
Most cited references9
- Record: found
- Abstract: not found
- Article: not found
A leptin missense mutation associated with hypogonadism and morbid obesity.
T Issad, L Camoin, Natalie A. Strobel … (1998)
- Record: found
- Abstract: found
- Article: not found
Crystal structure of the obese protein leptin-E100.
H H Hsiung, J Wery, J Beals … (1997)
- Record: found
- Abstract: found
- Article: not found
Biologically inactive leptin and early-onset extreme obesity.
Martin Wabitsch, Jan-Bernd Funcke, Belinda Lennerz … (2015)