- Record: found
- Abstract: found
- Article: found
Comparison of King Vision video laryngoscope and Macintosh laryngoscope: a prospective randomized controlled clinical trial Translated title: Comparação entre o videolaringoscópio King Vision e o laringoscópio Macintosh: um ensaio clínico prospectivo randomizado e controlado
Abstract
Background and objectives
We compared the efficiency of the King Vision video laryngoscope and the Macintosh laryngoscope, when used by experienced anesthesiologists on adult patients with varying intubating conditions, in a prospective randomized controlled clinical trial.
Methods
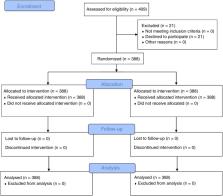
A total of 388 patients with an American Society of Anesthesiologists physical status of I or II, scheduled for general anesthesia with endotracheal intubation. Each patient was intubated with both laryngoscopes successively, in a randomized order. Intubation success rate, time to best glottic view, time to intubation, time to ventilation, Cormack–Lehane laryngoscopy grades, and complications related to the laryngoscopy and intubation were analyzed.
Results and conclusions
First pass intubation success rates were similar for the King Vision and the Macintosh (96.6% vs. 94.3%, respectively, p > 0.05). King Vision resulted in a longer average time to glottic view (95% CI 0.5–1.4 s, p < 0.001), and time to intubation (95% CI 3–4.6 s, p < 0.001). The difference in time to intubation was similar when unsuccessful intubation attempts were excluded (95% CI 2.8–4.4 s, p < 0.001). Based on the modified Mallampati class at the preoperative visit, the King Vision improved the glottic view in significantly more patients (220 patients, 56.7%) compared with the Macintosh (180 patients, 46.4%) ( p < 0.001). None of the patients had peripheral oxygen desaturation below 94%. Experienced anesthesiologists may obtain similar rates of first pass intubation success and airway trauma with both laryngoscopes. King Vision requires longer times to visualize the glottis and to intubate the trachea, but does not cause additional desaturation.
Resumo
Comparamos a eficiência do videolaringoscópio King Vision e do laringoscópio Macintosh, quando usados por anestesiologistas experientes em pacientes adultos com diferentes condições de intubação, em um estudo clínico prospectivo randomizado e controlado.
Foram selecionados 388 pacientes com estado físico ASA I ou II (de acordo com a classificação da American Society of Anesthesiologists – ASA), programados para anestesia geral com intubação traqueal. Cada paciente foi intubado com ambos os laringoscópios sucessivamente, em uma ordem aleatória. A taxa de sucesso da intubação, o tempo até a melhor visibilização da glote, o tempo de intubação, o tempo de ventilação, a classificação de Cormack-Lehane (graus) e as complicações relacionadas à laringoscopia e intubação foram analisados.
As taxas de sucesso na intubação na primeira tentativa foram similares para o King Vision e o Macintosh (96,6% vs. 94,3%, respectivamente, p > 0,05). As médias dos tempos até a melhor visibilização da glote (IC 95% 0,5–1,4s, p < 0,001) e de intubação (IC 95% 3–4,6s, p < 0,001) foram maiores no King Vision. A diferença no tempo de intubação foi semelhante quando as tentativas malsucedidas de intubação foram excluídas (IC 95% 2,8–4,4s, p < 0,001). Com base na classificação de Mallampati modificada na consulta pré-operatória, o King Vision melhorou significativamente a visibilização da glote em mais pacientes (220 pacientes, 56,7%) em comparação com o Macintosh (180 pacientes, 46,4%) ( p < 0,001). Nenhum dos pacientes apresentou dessaturação periférica de oxigênio abaixo de 94%. Os anestesiologistas experientes podem obter taxas semelhantes de sucesso na primeira tentativa de intubação e de traumas das vias aéreas com ambos os laringoscópios. O King Vision requer tempos mais longos até a visibilização da glote e de intubação traqueal, mas não causa dessaturação adicional.
Related collections
Most cited references27
- Record: found
- Abstract: not found
- Article: not found
Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway.
- Record: found
- Abstract: found
- Article: not found