- Record: found
- Abstract: found
- Article: found
Internal jugular vein duplication
letter
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Sir,
The internal jugular vein is the largest vein in the neck and drains the intracranial
structures and deep structures of the face and neck. It runs the length of the neck
slightly lateral to the common carotid artery within the carotid sheath and, on the
right, crosses in front of the right subclavian artery, to join the subclavian vein.[1]
Duplication of the internal jugular vein is a rare finding.
We came across a case of duplication of right internal jugular vein and offer some
clinical comments on the importance of this rare anatomical feature.
A 65-year-old woman with a T2N0M0 squamous cell carcinoma of the right margin of the
tongue had a local wide excision and an ipsilateral modified type 3 radical neck dissection.
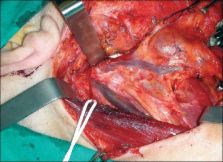
During the dissection of the neck a bifurcation of the right internal jugular vein,
about 2cm from the jugular foramen was encountered [Figure 1]. Both branches of the
internal jugular vein had the same thickness and poured into the right subclavian
vein. The anterior branch was parallel to the carotid artery and received the common
facial vein, the superior and inferior thyroid veins and the transverse cervical vein.
The posterior branch passed within the carotid sheath, drained only the cerebral blood
and emptied into the subclavian vein lateral to the medial branch. None showed evidence
of phlebectasia or aneurysm. The spinal accessory nerve passed between the medial
and lateral branches, exactly superficial to the medial branch and under the lateral
branch.
Figure 1
The bifurcation of the right internal jugular vein discovered during neck dissection
Duplication of the internal jugular vein is a rare congenital anomaly. The vein divides
into two branches that separately enter the subclavian vein. Almost always it involves
the upper third of the vein.[2
3] In our case, the duplication was 2 cm below the base of the skull.
Duplication of the internal jugular vein is usually reported in association with phlebectasia,
which is a soft non-pulsatile cervical swelling that increases in size during Valsalva
maneuver.[4] In our case, no aneurysm or phlebectasia was observed.
Three theories have been formulated to explain duplication:[3] the vascular theory,
that is usually accepted[3] the neural hypothesis and the bony hypothesis. Duplication
is thought to result from the appearance of a secondary venous ring at a lower level
surrounding the spinal accessory nerve during foetal life.[4] The persistence of this
secondary ring in adult life may be important in the aetiology of venous duplication.[4]
Unexpected duplication of the internal jugular vein could impact specific clinical
procedures, creating the possibility of either iatrogenic morbidity or incorrect diagnosis.
In our case, the large area involved and additional sites for ligature complicated
selective neck dissection.
Related collections
Most cited references4
- Record: found
- Abstract: found
- Article: not found
High duplication of the internal jugular vein: clinical incidence in the adult and surgical consequences, a report of three clinical cases.
J Prades, N Merzougui, J-M Dumollard … (2002)
- Record: found
- Abstract: found
- Article: not found
Bilateral duplicated internal jugular veins: case study and literature review.
N Mazurek, G J Lelonek, L Schalop … (2007)
- Record: found
- Abstract: found
- Article: not found
Duplication of internal jugular vein and relation to the spinal accessory nerve.
A Alaani, J Pracy, Lorraine Webster (2005)