- Record: found
- Abstract: found
- Article: found
The discrepancy between admission and discharge diagnoses: Underlying factors and potential clinical outcomes in a low socioeconomic country

Read this article at
Abstract
Objective
The discrepancy between admission and discharge diagnosis can lead to possible adverse patient outcomes. There are gaps in integrated studies, and less is understood about its characteristics and effects. Therefore, this study was conducted to determine the frequency, characteristics, and outcomes of diagnostic discrepancies at admission and discharge.
Design and data sources
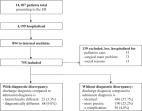
This retrospective study reviewed the admitting and discharge diagnoses of adult patients admitted at Aga Khan University Hospital (AKUH), Internal Medicine Department between October 2018 and February 2019. The frequency and outcomes of discrepancies in patient diagnoses were noted among Emergency Department (ED) physician versus admitting physician, admitting physician versus discharge physician, and ED physician versus discharge physician for the full match, partial match, and mismatch diagnoses. The studied outcomes included interdepartmental transfer, Intensive Care Unit (ICU) transfer, in-hospital mortality, readmission within 30 days, and the length of stay. For simplicity, we only analyzed the factors for the discrepancy among ED physicians and discharge physicians.
Results
Out of 537 admissions, there were 25.3–27.2% admissions with full match diagnoses while 18.6–19.4% and 45.3–47.9% had mismatch and partial match diagnoses respectively. The discrepancy resulted in an increased number of interdepartmental transfers (5–5.8%), ICU transfers (5.6–8.7%), in-hospital mortality (8–11%), and readmissions within 30 days in ED (14.4%-16.7%). A statistically significant difference was observed for the ward’s length of stay with the most prolonged stay in partially matched diagnoses (6.3 ± 5.4 days). Among all the factors that were evaluated for the diagnostic discrepancy, older age, multi-morbidities, level of trainee clerking the patient, review by ED faculty, incomplete history, and delay in investigations at ED were associated with significant discrepant diagnoses.
Conclusions
Diagnostic discrepancies are a relevant and significant healthcare problem. Fixed patient or physician characteristics do not readily predict diagnostic discrepancies. To reduce the diagnostic discrepancy, emphasis should be given to good history taking and thorough physical examination. Patients with older age and multi-morbidity should receive significant consideration.
Related collections
Most cited references15
- Record: found
- Abstract: found
- Article: not found
The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II.
- Record: found
- Abstract: found
- Article: not found
Change in the quality of care delivered to Medicare beneficiaries, 1998-1999 to 2000-2001.
- Record: found
- Abstract: found
- Article: found