- Record: found
- Abstract: found
- Article: found
A case of constrictive pericarditis due to angiosarcoma mimicking acute ST elevation myocardial infarction
other
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Constrictive pericarditis (CP) is a very rare condition, and its etiology is most
commonly idiopathic. Cardiac angiosarcoma (AS) is an exceptional tumor of heart but
is the most common primary cardiac malignant tumor in adults.
A 38-year-old male was referred to our clinic for substernal chest pain and dyspnea
for the last 3 months. He had developed these symptoms after a severe upper respiratory
tract infection. Physical examination revealed jugular venous distention, pericardial
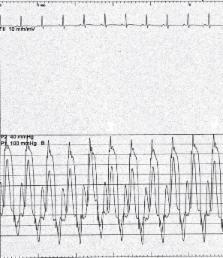
knock, hepatomegaly, and +1 pitting pretibial edema. His ECG showed newly developed
ST segment elevation on V1-6 (Fig. 1) consistent with anterior myocardial infarction.
Subsequent coronary angiography was normal (Fig. 2). Echocardiography showed thickened
pericardium (Fig. 3), septal bounce (Video 1, 2), and .25% increase in mitral E velocity
during expiration (Fig. 4).
Figure 1
ECG showed acute anterior myocardial infarction
Figure 2
(a) RAO caudal view showed normal LAD and Cx. (b) LAO view showed normal RCA
Figure 3
Parasternal long axis view showed thickened pericardium
Video 1
Video 2
Figure 4
Doppler echocardiography revealed ≥25% increase in mitral E velocity during expiration
(arrow showed expirium, spike showed inspirium)
Tissue Doppler examination revealed the presence of anulusus pardoxus (Fig. 5). Cardiac
MRI demonstrated thickened pericardium and septal bounce (Fig. 6). Cardiac catheterization
revealed a preserved x descent, a prominent y descent (Fig. 7), and an exaggerated
ventricular interaction (Fig. 8).
Figure 5
Tissue Doppler examination revealed anulusus pardoxus (arrow showed E’ velocity of
the lateral mitral annulus, spike showed E’ velocity of the septal mitral annulus)
Figure 6
Cardiac MRI demonstrate thickened pericardium
Figure 7
Preserved x descent and prominent y descent on right atrial pressure trace
Figure 8
Exaggerated ventricular interaction on ventricular pressure trace
Pericardiectomy was performed, and screening procedures for tuberculosis, viral-bacterial
or fungal infections, vasculitis, and connective tissue disease revealed negative
results. Pathological examination of pericardiectomy preparates showed spindle-shaped
cells, which was consistent with angiosarcoma (Fig. 9). PET-CT showed increased metabolic
activity on pericardial surface (Fig. 10).
Figure 9
Pericardiectomy preparates showed spindle-shaped cells, which was consistent with
angiosarcoma
Figure 10
PET CT showed increased metabolic activity on pericardial surface
CP is a rare disease and is the end stage of an inflammatory process involving the
pericardium. Primary cardiac AS is exceptional tumor. Pericardium involvement may
be seen in cardiac AS; however, there is no literature regarding CP. To our knowledge,
this case is the first presentation of CP due to cardiac AS.
Video 1
Parasternal short-axis view showed septal bounce.
Video 2
Apical four-chamber view showed septal bounce.