- Record: found
- Abstract: found
- Article: found
Multifactorial QT Interval Prolongation and Takotsubo Cardiomyopathy
Read this article at
Abstract
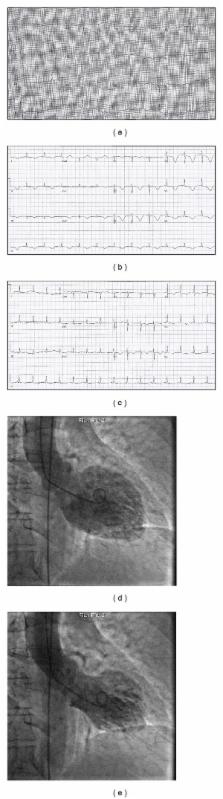
A 71-year-old woman collapsed while working as a grocery store cashier. CPR was performed and an AED revealed torsades de pointes (TdP). She was subsequently defibrillated resulting in restoration of sinus rhythm with a QTc interval of 544 msec. Further evaluation revealed a diagnosis of Takotsubo Cardiomyopathy (TCM) contributing to the development of a multifactorial acquired long QT syndrome (LQTS). The case highlights the role of TCM as a cause of LQTS in the setting of multiple risk factors including old age, female gender, hypokalemia, and treatment with QT prolonging medications. It also highlights the multifactorial nature of acquired LQTS and lends support to growing evidence of an association with TCM.
Related collections
Most cited references11
- Record: found
- Abstract: found
- Article: not found
Acquired long QT syndrome from stress cardiomyopathy is associated with ventricular arrhythmias and torsades de pointes.
- Record: found
- Abstract: not found
- Article: not found
Clinical and genetic determinants of torsade de pointes risk.
- Record: found
- Abstract: found
- Article: not found