- Record: found
- Abstract: found
- Article: not found
Four-flap Breast Reconstruction: Bilateral Stacked DIEP and PAP Flaps
Read this article at

Abstract
Background:
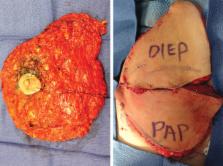
In cases of bilateral breast reconstruction when the deep inferior epigastric perforator (DIEP) free flap alone does not provide sufficient volume for body-specific reconstruction, stacking each DIEP flap with a second free flap will deliver added volume and maintain a purely autologous reconstruction. Stacking the profunda artery perforator (PAP) flap with the DIEP flap offers favorable aesthetics and ideal operative efficiency. We present the indications, technique, and outcomes of our experience with 4-flap breast reconstruction using stacked DIEP/PAP flaps.
Methods:
The authors performed 4-flap DIEP/PAP breast reconstruction in 20 patients who required bilateral reconstruction without adequate single donor flap volume. The timing of reconstruction, average mastectomy/flap weights, and operative time are reported. Complications reviewed include fat necrosis, dehiscence, hematoma, seroma, mastectomy flap necrosis, and flap loss.
Results:
Twenty patients underwent 4-flap DIEP/PAP breast reconstruction. Surgical time averaged 7 hours and 20 minutes. The primary recipient vessels were the antegrade and retrograde internal mammary vessels. No flap losses occurred. Complications included 1 hematoma, 1 incidence of arterial and venous thrombosis successfully treated with anastomotic revision, 1 incidence of thigh donor site dehiscence, and 3 episodes of minor mastectomy skin flap necrosis.
Conclusions:
Four-flap breast reconstruction is a favorable autologous reconstructive option for patients requiring bilateral reconstruction without adequate single donor flap volume. Stacking DIEP/PAP flaps as described is both safe and efficient. Furthermore, this combination provides superior aesthetics mirroring the natural geometry of the breast. Bilateral stacked DIEP/PAP flaps represent our first choice for breast reconstruction in this patient population.
Related collections
Most cited references21
- Record: found
- Abstract: found
- Article: not found
Increasing rates of contralateral prophylactic mastectomy among patients with ductal carcinoma in situ.
- Record: found
- Abstract: found
- Article: not found
A 10-year retrospective review of 758 DIEP flaps for breast reconstruction.
- Record: found
- Abstract: found
- Article: not found