- Record: found
- Abstract: found
- Article: found
Improving the implementation of health workforce policies through governance: a review of case studies
Read this article at
Abstract
Introduction
Responsible governance is crucial to national development and a catalyst for achieving the Millennium Development Goals. To date, governance seems to have been a neglected issue in the field of human resources for health (HRH), which could be an important reason why HRH policy formulation and implementation is often poor. This article aims to describe how governance issues have influenced HRH policy development and to identify governance strategies that have been used, successfully or not, to improve HRH policy implementation in low- and middle-income countries (LMIC).
Methods
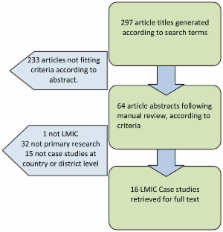
We performed a descriptive literature review of HRH case studies which describe or evaluate a governance-related intervention at country or district level in LMIC. In order to systematically address the term 'governance' a framework was developed and governance aspects were regrouped into four dimensions: 'performance', 'equity and equality', 'partnership and participation' and 'oversight'.
Results and discussion
In total 16 case studies were included in the review and most of the selected studies covered several governance dimensions. The dimension 'performance' covered several elements at the core of governance of HRH, decentralization being particularly prominent. Although improved equity and/or equality was, in a number of interventions, a goal, inclusiveness in policy development and fairness and transparency in policy implementation did often not seem adequate to guarantee the corresponding desirable health workforce scenario. Forms of partnership and participation described in the case studies are numerous and offer different lessons. Strikingly, in none of the articles was 'partnerships' a core focus. A common theme in the dimension of 'oversight' is local-level corruption, affecting, amongst other things, accountability and local-level trust in governance, and its cultural guises. Experiences with accountability mechanisms for HRH policy development and implementation were lacking.
Conclusion
This review shows that the term 'governance' is neither prominent nor frequent in recent HRH literature. It provides initial lessons regarding the influence of governance on HRH policy development and implementation. The review also shows that the evidence base needs to be improved in this field in order to better understand how governance influences HRH policy development and implementation. Tentative lessons are discussed, based on the case studies.
Related collections
Most cited references19
- Record: found
- Abstract: found
- Article: not found
Framework for assessing governance of the health system in developing countries: gateway to good governance.

- Record: found
- Abstract: found
- Article: found
Strategic management of the health workforce in developing countries: what have we learned?
- Record: found
- Abstract: found
- Article: not found