- Record: found
- Abstract: found
- Article: found
A Systematic Review of Studies Eliciting Willingness-to-Pay per Quality-Adjusted Life Year: Does It Justify CE Threshold?
Read this article at
Abstract
Background
A number of studies have been conducted to estimate willingness to pay (WTP) per quality-adjusted life years (QALY) in patients or general population for various diseases. However, there has not been any systematic review summarizing the relationship between WTP per QALY and cost-effectiveness (CE) threshold based on World Health Organization (WHO) recommendation.
Objective
To systematically review willingness-to-pay per quality-adjusted-life-year (WTP per QALY) literature, to compare WTP per QALY with Cost-effectiveness (CE) threshold recommended by WHO, and to determine potential influencing factors.
Methods
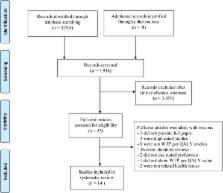
We searched MEDLINE, EMBASE, Psyinfo, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Center of Research Dissemination (CRD), and EconLit from inception through 15 July 2014. To be included, studies have to estimate WTP per QALY in health-related issues using stated preference method. Two investigators independently reviewed each abstract, completed full-text reviews, and extracted information for included studies. We compared WTP per QALY to GDP per capita, analyzed, and summarized potential influencing factors.
Results
Out of 3,914 articles founded, 14 studies were included. Most studies (92.85%) used contingent valuation method, while only one study used discrete choice experiments. Sample size varied from 104 to 21,896 persons. The ratio between WTP per QALY and GDP per capita varied widely from 0.05 to 5.40, depending on scenario outcomes (e.g., whether it extended/saved life or improved quality of life), severity of hypothetical scenarios, duration of scenario, and source of funding. The average ratio of WTP per QALY and GDP per capita for extending life or saving life (2.03) was significantly higher than the average for improving quality of life (0.59) with the mean difference of 1.43 (95% CI, 1.81 to 1.06).
Conclusion
This systematic review provides an overview summary of all studies estimating WTP per QALY studies. The variation of ratio of WTP per QALY and GDP per capita depended on several factors may prompt discussions on the CE threshold policy. Our research work provides a foundation for defining future direction of decision criteria for an evidence-informed decision making system.
Related collections
Most cited references40
- Record: found
- Abstract: found
- Article: not found
Assessing cost-effectiveness in healthcare: history of the $50,000 per QALY threshold.
- Record: found
- Abstract: found
- Article: not found
Use of cost-effectiveness analysis in health-care resource allocation decision-making: how are cost-effectiveness thresholds expected to emerge?
- Record: found
- Abstract: found
- Article: not found