- Record: found
- Abstract: found
- Article: found
Evaluating the impact of alcohol minimum unit pricing on deaths and hospitalisations in Scotland: a controlled interrupted time series study
Read this article at
Summary
Background
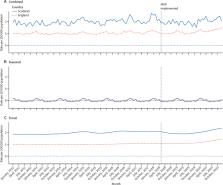
Since May 1, 2018, every alcoholic drink sold in Scotland has had minimum unit pricing (MUP) of £0·50 per unit. Previous studies have indicated that the introduction of this policy reduced alcohol sales by 3%. We aimed to assess whether this has led to reductions in alcohol-attributable deaths and hospitalisations.
Methods
Study outcomes, wholly attributable to alcohol consumption, were defined using routinely collected data on deaths and hospitalisations. Controlled interrupted time series regression was used to assess the legislation's impact in Scotland, and any effect modification across demographic and socioeconomic deprivation groups. The pre-intervention time series ran from Jan 1, 2012, to April 30, 2018, and for 32 months after the policy was implemented (until Dec 31, 2020). Data from England, a part of the UK where the intervention was not implemented, were used to form a control group.
Findings
MUP in Scotland was associated with a significant 13·4% reduction (95% CI –18·4 to –8·3; p=0·0004) in deaths wholly attributable to alcohol consumption. Hospitalisations wholly attributable to alcohol consumption decreased by 4·1% (–8·3 to 0·3; p=0·064). Effects were driven by significant improvements in chronic outcomes, particularly alcoholic liver disease. Furthermore, MUP legislation was associated with a reduction in deaths and hospitalisations wholly attributable to alcohol consumption in the four most socioeconomically deprived deciles in Scotland.
Interpretation
The implementation of MUP legislation was associated with significant reductions in deaths, and reductions in hospitalisations, wholly attributable to alcohol consumption. The greatest improvements were in the four most socioeconomically deprived deciles, indicating that the policy is positively tackling deprivation-based inequalities in alcohol-attributable health harm.
Related collections
Most cited references31
- Record: found
- Abstract: found
- Article: not found
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies.

- Record: found
- Abstract: found
- Article: found
Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019
- Record: found
- Abstract: found
- Article: not found