- Record: found
- Abstract: found
- Article: found
Hyaluronic acid-carboxymethylcellulose reduced postoperative bowel adhesions following laparoscopic urologic pelvic surgery: a prospective, randomized, controlled, single-blind study
Read this article at
Abstract
Background
To assess the anti-adhesive effect of treatment with hyaluronic acid-carboxymethylcellulose following laparoscopic radical prostatectomy.
Methods
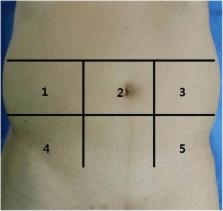
This was a randomized, controlled, single-blind, parallel-group study using hyaluronic acid-carboxymethylcellulose in patients who underwent laparoscopic radical prostatectomy. Sixty patients were enrolled in the study. All patients were randomly assigned to either the hyaluronic acid-carboxymethylcellulose treatment group ( n = 30) or the control group ( n = 30). Viscera slide ultrasounds and plain X-rays were obtained at enrollment (V0), postoperative week 12 (V1), and 24 (V2). The primary end point was the difference in the excursion distance in the viscera slide ultrasound between V0 and V2.
Results
A total of 50 patients completed this study. The average excursion distance at V2 in the experimental group ( n = 25) was significantly longer than in the control group ( n = 25, 2.7 ± 1.2 vs. 1.3 ± 1.0 cm, respectively; p < 0.001). The differences in the V0 and V2 excursion distances were significantly higher in the control group than in the experimental group (1.48 ± 1.5 vs. 2.9 ± 1.2 cm, respectively; p < 0.001). None of patients showed adverse events associated with the use of hyaluronic acid-carboxymethylcellulose.
Related collections
Most cited references20
- Record: found
- Abstract: found
- Article: not found
Pathophysiology and prevention of postoperative peritoneal adhesions.
- Record: found
- Abstract: found
- Article: not found
Intestinal obstruction from adhesions--how big is the problem?
- Record: found
- Abstract: found
- Article: not found