- Record: found
- Abstract: found
- Article: found
Incidence and Risk Factors for Neonatal Tetanus in Admissions to Kilifi County Hospital, Kenya
Read this article at
Abstract
Background
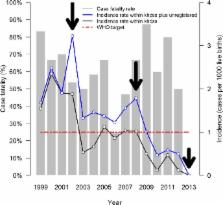
Neonatal Tetanus (NT) is a preventable cause of mortality and neurological sequelae that occurs at higher incidence in resource-poor countries, presumably because of low maternal immunisation rates and unhygienic cord care practices. We aimed to determine changes in the incidence of NT, characterize and investigate the associated risk factors and mortality in a prospective cohort study including all admissions over a 15-year period at a County hospital on the Kenyan coast, a region with relatively high historical NT rates within Kenya.
Methods
We assessed all neonatal admissions to Kilifi County Hospital in Kenya (1999–2013) and identified cases of NT (standard clinical case definition) admitted during this time. Poisson regression was used to examine change in incidence of NT using accurate denominator data from an area of active demographic surveillance. Logistic regression was used to investigate the risk factors for NT and factors associated with mortality in NT amongst neonatal admissions. A subset of sera from mothers (n = 61) and neonates (n = 47) were tested for anti-tetanus antibodies.
Results
There were 191 NT admissions, of whom 187 (98%) were home deliveries. Incidence of NT declined significantly (Incidence Rate Ratio: 0.85 (95% Confidence interval 0.81–0.89), P<0.001) but the case fatality (62%) did not change over the study period (P = 0.536). Younger infant age at admission (P = 0.001) was the only independent predictor of mortality. Compared to neonatal hospital admittee controls, the proportion of home births was higher among the cases. Sera tested for antitetanus antibodies showed most mothers (50/61, 82%) had undetectable levels of antitetanus antibodies, and most (8/9, 89%) mothers with detectable antibodies had a neonate without protective levels.
Related collections
Most cited references33
- Record: found
- Abstract: found
- Article: not found
4 million neonatal deaths: when? Where? Why?
- Record: found
- Abstract: found
- Article: not found
Placental transport of immunoglobulin G

- Record: found
- Abstract: found
- Article: found