- Record: found
- Abstract: found
- Article: found
Use of Telemedicine and Quality of Care Among Medicare Enrollees With Serious Mental Illness
Read this article at
Abstract
This cohort study examines the use of telemental health services by Medicare beneficiaries with schizophrenia or bipolar I disorder, and whether outcomes differ according to a practice’s extent of telemedicine use.
Key Points
Question
Was telemedicine use during the COVID-19 pandemic associated with more visits and higher quality of care for patients with serious mental illness?
Findings
In this cohort study of 120 050 Medicare beneficiaries with schizophrenia or bipolar I disorder, patients receiving mental health care at practices that almost exclusively switched to telemental health service had 13.0% more mental health visits than those receiving care at practices that largely used in-person visits. There were no changes in medication adherence, hospital and emergency department use, or mortality based on the extent of telemental health use.
Abstract
Importance
During the COVID-19 pandemic, a large fraction of mental health care was provided via telemedicine. The implications of this shift in care for use of mental health service and quality of care have not been characterized.
Objective
To compare changes in care patterns and quality during the first year of the pandemic among Medicare beneficiaries with serious mental illness (schizophrenia or bipolar I disorder) cared for at practices with higher vs lower telemedicine use.
Design, Setting, and Participants
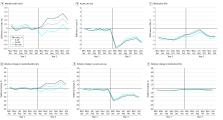
In this cohort study, Medicare fee-for-service beneficiaries with schizophrenia or bipolar I disorder were attributed to specialty mental health practices that delivered the majority of their mental health care in 2019. Practices were categorized into 3 groups based on the proportion of telemental health visits provided during the first year of the pandemic (March 2020-February 2021): lowest use (0%-49%), middle use (50%-89%), or highest use (90%-100%). Across the 3 groups of practices, differential changes in patient outcomes were calculated from the year before the pandemic started to the year after. These changes were also compared with differential changes from a 2-year prepandemic period. Analyses were conducted in November 2022.
Main Outcomes and Measures
The primary outcome was the total number of mental health visits (telemedicine plus in-person) per person. Secondary outcomes included the number of acute hospital and emergency department encounters, all-cause mortality, and quality outcomes, including adherence to antipsychotic and mood-stabilizing medications (as measured by the number of months of medication fills) and 7- and 30-day outpatient follow-up rates after discharge for a mental health hospitalization.
Results
The pandemic cohort included 120 050 Medicare beneficiaries (mean [SD] age, 56.5 [14.5] years; 66 638 females [55.5%]) with serious mental illness. Compared with prepandemic changes and relative to patients receiving care at practices with the lowest telemedicine use: patients receiving care at practices in the middle and highest telemedicine use groups had 1.11 (95% CI, 0.45-1.76) and 1.94 (95% CI, 1.28-2.59) more mental health visits per patient per year (or 7.5% [95% CI, 3.0%-11.9%] and 13.0% [95% CI, 8.6%-17.4%] more mental health visits per year, respectively). Among patients of practices with middle and highest telemedicine use, changes in adherence to antipsychotic and mood-stabilizing medications were −0.4% (95% CI, −1.3% to 0.5%) and −0.1% (95% CI, −1.0% to 0.8%), and hospital and emergency department use for any reason changed by 2.4% (95% CI, −1.5% to 6.2%) and 2.8% (95% CI, −1.2% to 6.8%), respectively. There were no significant differential changes in postdischarge follow-up or mortality rates according to the level of telemedicine use.
Conclusions and Relevance
In this cohort study of Medicare beneficiaries with serious mental illness, patients receiving care from practices that had a higher level of telemedicine use during the COVID-19 pandemic had more mental health visits per year compared with prepandemic levels, with no differential changes in other observed quality metrics over the same period.
Related collections
Most cited references37
- Record: found
- Abstract: found
- Article: not found
The effectiveness of telemental health: a 2013 review.
- Record: found
- Abstract: found
- Article: found
The COVID-19 Global Pandemic: Implications for People With Schizophrenia and Related Disorders
- Record: found
- Abstract: found
- Article: not found