- Record: found
- Abstract: found
- Article: found
Eosinophilic granulomatosis with polyangiitis: myocardial thickening reversed by corticosteroids
Read this article at
Abstract
Background
In 1951 Churg and Strauss first described the clinical condition now known as eosinophilic granulomatosis with polyangiitis (EGPA), characterized by asthma, nasal polyposis, rhinosinusitis, hypereosinophilia with organ infiltration, and necrotizing vasculitis. It is classified as an antineutrophil cytoplasmic antibody (ANCA) associated vasculitis, but ANCA negativity is common and more frequently encountered in EGPA with myocardial involvement. Long-term survival has substantially improved with corticosteroid treatment but myocardial involvement is still the leading cause of death in EGPA.
Case presentation
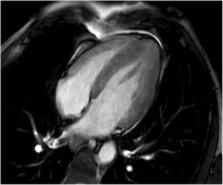
A 53-year old man with a history of asthma and nasal polyposis presented with acute chest pain and elevated troponin; a percutaneous coronary intervention was performed. The left ventricle was described as hypertrophic. After 20 days the myocardium had markedly increased in thickness of both the right and left ventricle. Evaluation revealed hypereosinophilia in the blood and nasal mucosal tissue, which confirmed the diagnosis of EGPA. He presented with signs of active vasculitis including weight loss, tiredness, intracerebral hemorrhage, and increasing serum creatinine. After 6 days of corticosteroid treatment, the myocardium returned to its initial thickness.
Related collections
Most cited references15
- Record: found
- Abstract: found
- Article: not found
Eosinophilic granulomatosis with polyangiitis (Churg-Strauss) (EGPA) Consensus Task Force recommendations for evaluation and management.
- Record: found
- Abstract: found
- Article: not found
Prevalence and clinical significance of antineutrophil cytoplasmic antibodies in Churg-Strauss syndrome.
- Record: found
- Abstract: found
- Article: not found