- Record: found
- Abstract: found
- Article: found
2020 APHRS/HRS expert consensus statement on the investigation of decedents with sudden unexplained death and patients with sudden cardiac arrest, and of their families
Read this article at
Abstract
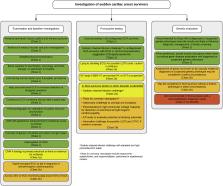
This international multidisciplinary document intends to provide clinicians with evidence-based practical patient-centered recommendations for evaluating patients and decedents with (aborted) sudden cardiac arrest and their families. The document includes a framework for the investigation of the family allowing steps to be taken, should an inherited condition be found, to minimize further events in affected relatives. Integral to the process is counseling of the patients and families, not only because of the emotionally charged subject, but because finding (or not finding) the cause of the arrest may influence management of family members. The formation of multidisciplinary teams is essential to provide a complete service to the patients and their families, and the varied expertise of the writing committee was formulated to reflect this need. The document sections were divided up and drafted by the writing committee members according to their expertise. The recommendations represent the consensus opinion of the entire writing committee, graded by Class of Recommendation and Level of Evidence. The recommendations were opened for public comment and reviewed by the relevant scientific and clinical document committees of the Asia Pacific Heart Rhythm Society (APHRS) and the Heart Rhythm Society (HRS); the document underwent external review and endorsement by the partner and collaborating societies. While the recommendations are for optimal care, it is recognized that not all resources will be available to all clinicians. Nevertheless, this document articulates the evaluation that the clinician should aspire to provide for patients with sudden cardiac arrest, decedents with sudden unexplained death, and their families.
Related collections
Most cited references361
- Record: found
- Abstract: not found
- Article: not found
2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC).
- Record: found
- Abstract: found
- Article: not found