- Record: found
- Abstract: found
- Article: found
Comparative trends in coronary heart disease subgroup hospitalisation rates in England and Australia
Read this article at
Abstract
Background
Population-based coronary heart disease (CHD) studies have focused on myocardial infarction (MI) with limited data on trends across the spectrum of CHD. We investigated trends in hospitalisation rates for acute and chronic CHD subgroups in England and Australia from 1996 to 2013.
Methods
CHD hospitalisations for individuals aged 35–84 years were identified from electronic hospital data from 1996 to 2013 for England and Australia and from the Oxford Region and Western Australia. CHD subgroups identified were acute coronary syndromes (ACS) (MI and unstable angina) and chronic CHD (stable angina and ‘other CHD’). We calculated age-standardised and age-specific rates and estimated annual changes (95% CI) from age-adjusted Poisson regression.
Results
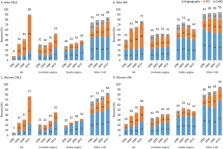
From 1996 to 2013, there were 4.9 million CHD hospitalisations in England and 2.6 million in Australia (67% men). From 1996 to 2003, there was between-country variation in the direction of trends in ACS and chronic CHD hospitalisation rates (p<0.001). During 2004–2013, reductions in ACS hospitalisation rates were greater than for chronic CHD hospitalisation rates in both countries, with the largest subgroup declines in unstable angina (England: men: −7.1 %/year, 95% CI −7.2 to –7.0; women: −7.5 %/year, 95% CI −7.7 to –7.3; Australia: men: −8.5 %/year, 95% CI −8.6 to –8.4; women: −8.6 %/year, 95% CI −8.8 to –8.4). Other CHD rates increased in individuals aged 75–84 years in both countries. Chronic CHD comprised half of all CHD admissions, with the majority involving angiography or percutaneous coronary intervention.
Related collections
Most cited references20
- Record: found
- Abstract: found
- Article: not found
Explaining the decline in coronary heart disease mortality in England and Wales between 1981 and 2000.
- Record: found
- Abstract: found
- Article: not found
Twenty-two-year trends in incidence of myocardial infarction, coronary heart disease mortality, and case fatality in 4 US communities, 1987-2008.
- Record: found
- Abstract: not found
- Article: not found