- Record: found
- Abstract: found
- Article: found
Treatment of Proximal Trochlear Dysplasia in the Setting of Patellar Instability: An Arthroscopic Technique
Read this article at
Abstract
Patellar instability is a complex disorder with multiple etiologies, and treatment must be individualized to the unique pathoanatomy of each patient. Medial patellofemoral ligament reconstruction is one of the most commonly performed procedures for the treatment of patellar instability. Patients with a symptomatic supratrochlear spur, defined by the presence of a “jumping” J sign on examination, also may benefit from an adjunctive proximal trochlear resection. Here, we describe a technique for an arthroscopic proximal trochlear resection, or “bumpectomy,” involving resection of the supratrochlear spur. In appropriately indicated patients, we have found this procedure to be a useful adjunct to medial patellofemoral ligament reconstruction without the need for concurrent trochlear sulcus deepening.
Technique Video
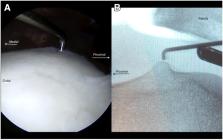
This is a presentation of an arthroscopic technique for proximal trochlear resection to treat patients with patellar instability. Our disclosures are listed here as well as online. This is a 17-year-old male patient who has a 10-year history of patellar instability with subluxation and occasional complete dislocation events laterally and failed conservative management. He has no effusion on examination, he has 2 quadrants of lateral and medial translation, and has a jumping J-sign that is 2 quadrants when going from extension to flexion. When we look at his lateral radiograph as well as 3-dimensional MRI data, we see that he has a 9.9-mm supratrochlear spur that is even greater than this when we add cartilage into the equation. We also see that this extension of the trochlea is proximal to the proximal aspect of the posterior condyles, which means that this is taller than the normal trochlear height and likely can be resected as opposed to a formal trochleoplasty being performed. The patient has a Caton–Deschamps ratio of 1.25, and a Dejour classification of B. We elected to treat the primary issues, which were the proximal bump as well as the ligamentous instability by performing a proximal trochlear resection and MPFL reconstruction with hamstring allograft. During the examination under anesthesia, we see a giant jumping J-sign as he gets to approximately 70° of flexion or slightly more. We then can evaluate lateral translation, where we see that he's fully dislocatable on extension and once he is fully dislocated, he has a difficult time engaging due to this area of abrupt transition as he gets into high flexion. If we move the knee into flexion and try to dislocate laterally at 90° this is not possible, but the kneecap does come out at about 70°, demonstrating his significant dysplasia. Arthroscopic examination, starting at the notch moving proximal, demonstrates the trochlear dysplasia as well as the supratrochlear spur that is present at the most proximal aspect of the trochlea. We now spinal needle localize a superior lateral patellar portal, which can help with diagnostic arthroscopy as well as visualization of this spur. Here we can see the superior lateral trochlear damage, as well as the patella tracking and the distal medial patellar chondral wear. We then obtain a perfect lateral radiograph, where here we can see on live fluoroscopy the prominence of this bump proximally. We then find the associated area in the arthroscopic view that correlates with the fluoroscopic view so that we know where to perform our resection. This bump is typically proximal to the posterior condyle line that we draw perpendicular to the femur, as discussed in the preoperative planning. We then postage stamp using fluoroscopy to demonstrate where this should be located so we know where to start our resection. We then use a combination of direct arthroscopic visualization as well as fluoroscopic visualization to use a curette to remove the proximal bump or spur. Once we are through the cartilage, we then move to a bone-cutting shaver, or a Burr, to resect this to the level of the anterior femur. The goal of the surgery is to create a smooth transition similar to a cam resection for hip arthroscopy which would allow for less contact pressure on the patella. Here we see spinal needle localization of the direct lateral portal; we can use this for easier access to resect the remaining component of the spur perpendicular to where the spur is located. It's important to carry this resection from all the way lateral to medial. We can then move our camera to the superior lateral portal and have our shaver through the direct lateral portal so that we can visualize the resection from another viewpoint to make sure that it is adequate. Using different portals for viewing as well as the fluoroscopic guidance helps make sure that the resection is being performed in a 3-dimensional way that is correct and allows for a smooth transition for the patella after this is complete. Resection of the bump is typically not adequate in itself, but the resection should be done in a way that the ramp that is created is relatively shallow and so that there is not a vertical wall that is created from the resection of the bump. Here we can see that smooth transition both in arthroscopy and now the final result on fluoroscopy here where it has been resected and there’s a normal transition into the groove. After surgery the patient’s allowed full weight-bearing in a brace locked in extension until they have active quad extension without a lag. We then unlock the brace, we work on full range of motion without restriction, and hope to achieve this by 6 to 8 weeks after surgery and allowing return to full activity 4 to 6 months after surgery. (MPFL, medial patellofemoral ligament reconstruction; MRI, magnetic resonance imaging.)
Related collections
Most cited references28
- Record: found
- Abstract: found
- Article: not found
Osteotomies in patello-femoral instabilities.
- Record: found
- Abstract: found
- Article: not found
The prevalence and combined prevalences of anatomic factors associated with recurrent patellar dislocation: a magnetic resonance imaging study.
- Record: found
- Abstract: found
- Article: not found