
- Record: found
- Abstract: found
- Article: found
Supply kits for antenatal and childbirth care during antenatal care and delivery: a mixed-methods systematic review, the qualitative approach.
Read this article at
Abstract
Antenatal care reduces maternal and perinatal mortality and morbidity through the detection and treatment of some conditions, but its coverage is less than optimal within certain populations. Supply kits for maternal health were designed to overcome barriers present when providing care during pregnancy and childbirth particularly to women from underserved population.
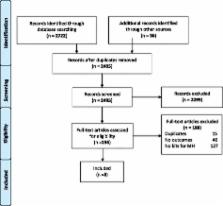
We conducted a mixed-methods systematic review on the use of supply kits. This manuscript presents the findings from qualitative studies that reported barriers, facilitators, and user’s recommendation in the adoption and implementation of any type of kit designed to be used during pregnancy or childbirth.
This review included eight studies, and seven were implemented in developing countries. Most studies assessed the implementation of clean delivery kits to be used during labour and delivery, and contributed to gain insights into factors that may hinder or foster the use of kits.
Clean delivery kits were conceived to cope with barriers related mainly to access. The most important barrier identified were those related to the socio-cultural and the lack of knowledge dimension such as who held the decision-making authority in the household, as well as popular beliefs behind the idea that birth preparation could bring bad luck, may prevent clients from adhering to their use. In addition, financial constraints and limited understanding of the instructions of use were accessibility barriers found. On the other hand, once used, clean delivery kits for maternal health were accepted by women and health workers. Convenience, hygienic components, and avoidance of delays in receiving care were viewed as satisfactory features.
Supply kits are mostly affordable and easily deployable. Increasing awareness among the population about the offered kits and providing information on their benefits emerges as a critical step to foster use in settings where kits are available. Implementation of this strategy requires low complexity resources and could make the use of kits an accepted alternative to increase the use of evidence-based interventions and thus improve quality of care during pregnancy, childbirth and neonatal period mainly at the community level in low income countries and remote areas with low access.
Related collections
Most cited references18
- Record: found
- Abstract: found
- Article: not found
Health service coverage and its evaluation.
- Record: found
- Abstract: found
- Article: found
WHO systematic review of maternal morbidity and mortality: the prevalence of severe acute maternal morbidity (near miss)

- Record: found
- Abstract: found
- Article: found