- Record: found
- Abstract: found
- Article: found
Serum procalcitonin elevation in critically ill patients at the onset of bacteremia caused by either gram negative or gram positive bacteria
Read this article at
Abstract
Background
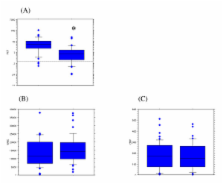
In the ICU, bacteremia is a life-threatening infection whose prognosis is highly dependent on early recognition and treatment with appropriate antibiotics. Procalcitonin levels have been shown to distinguish between bacteremia and noninfectious inflammatory states accurately and quickly in critically ill patients. However, we still do not know to what extent the magnitude of PCT elevation at the onset of bacteremia varies according to the Gram stain result.
Methods
Review of the medical records of every patient treated between May, 2004 and December, 2006 who had bacteremia caused by either Gram positive (GP) or Gram negative (GN) bacteria, and whose PCT dosage at the onset of infection was available.
Results
97 episodes of either GN bacteremia ( n = 52) or GP bacteremia ( n = 45) were included. Procalcitonin levels were found to be markedly higher in patients with GN bacteremia than in those with GP bacteremia, whereas the SOFA score value in the two groups was similar. Moreover, in the study population, a high PCT value was found to be independently associated with GN bacteremia. A PCT level of 16.0 ng/mL yielded an 83.0% positive predictive value and a 74.0% negative predictive value for GN-related bacteremia in the study cohort (AUROCC = 0.79; 95% CI, 0.71–0.88).
Related collections
Most cited references29
- Record: found
- Abstract: found
- Article: not found
Diagnostic value of procalcitonin, interleukin-6, and interleukin-8 in critically ill patients admitted with suspected sepsis.
- Record: found
- Abstract: found
- Article: not found
Procalcitonin as a diagnostic test for sepsis in critically ill adults and after surgery or trauma: a systematic review and meta-analysis.
- Record: found
- Abstract: found
- Article: not found