- Record: found
- Abstract: found
- Article: not found
World-wide, mortality is a high risk soon after initiation of hemodialysis
Read this article at

Abstract
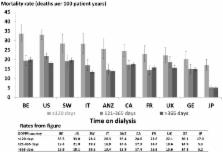
Mortality rates for maintenance hemodialysis patients are much higher than the general population and are even greater soon after starting dialysis. Here we analyzed mortality patterns in 86,886 patients in 11 countries focusing on the early dialysis period using data from the Dialysis Outcomes and Practice Patterns Study; a prospective cohort study of in-center hemodialysis. The primary outcome was all-cause mortality, using time-dependent Cox regression, stratified by study phase adjusted for age, sex, race, and diabetes. The main predictor was time since dialysis start as divided into early (up to 120 days), intermediate (121–365 days), and late (over 365 days) periods. Mortality rates (deaths/100 patient-years) were 26.7 (95% confidence intervals 25.6, 27.9), 16.9 (16.2, 17.6), and 13.7 (13.5, 14.0) in the early, intermediate, and late periods, respectively. In each country, mortality was higher in the early compared to the intermediate period with an adjusted range from 3.10 (2.22, 4.32) in Japan to 1.15 (0.87, 1.53) in the United Kingdom. Adjusted mortality rates were similar for intermediate and late periods. The ratio of elevated mortality rates in the early to the intermediate period increased with age. Within each period, mortality was higher in the United States than in most other countries. Thus, internationally, the early hemodialysis period is a high-risk time for all countries studied, with substantial differences in mortality between countries. Efforts to improve outcomes should focus on the transition period and first few months of dialysis.
Related collections
Most cited references41
- Record: found
- Abstract: found
- Article: not found
Predictors of early mortality among incident US hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS).
- Record: found
- Abstract: found
- Article: not found
Association of comorbid conditions and mortality in hemodialysis patients in Europe, Japan, and the United States: the Dialysis Outcomes and Practice Patterns Study (DOPPS).

- Record: found
- Abstract: found
- Article: found