- Record: found
- Abstract: found
- Article: found
Implications of early and guideline adherent physical therapy for low back pain on utilization and costs
Read this article at
Abstract
Background
Initial management decisions following a new episode of low back pain (LBP) are thought to have profound implications for health care utilization and costs. The purpose of this study was to evaluate the impact of early and guideline adherent physical therapy for low back pain on utilization and costs within the Military Health System (MHS).
Methods
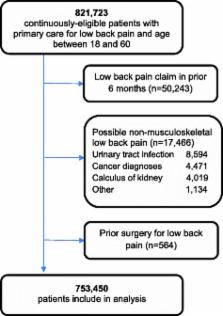
Patients presenting to a primary care setting with a new complaint of LBP from January 1, 2007 to December 31, 2009 were identified from the MHS Management Analysis and Reporting Tool. Descriptive statistics, utilization, and costs were examined on the basis of timing of referral to physical therapy and adherence to practice guidelines over a 2-year period. Utilization outcomes (advanced imaging, lumbar injections or surgery, and opioid use) were compared using adjusted odds ratios with 99% confidence intervals. Total LBP-related health care costs over the 2-year follow-up were compared using linear regression models.
Results
753,450 eligible patients with a primary care visit for LBP between 18–60 years of age were considered. Physical therapy was utilized by 16.3% (n = 122,723) of patients, with 24.0% (n = 17,175) of those receiving early physical therapy that was adherent to recommendations for active treatment. Early referral to guideline adherent physical therapy was associated with significantly lower utilization for all outcomes and 60% lower total LBP-related costs.
Conclusions
The potential for cost savings in the MHS from early guideline adherent physical therapy may be substantial. These results also extend the findings from similar studies in civilian settings by demonstrating an association between early guideline adherent care and utilization and costs in a single payer health system. Future research is necessary to examine which patients with LBP benefit early physical therapy and determine strategies for providing early guideline adherent care.
Related collections
Most cited references32
- Record: found
- Abstract: found
- Article: not found
Expenditures and health status among adults with back and neck problems.
- Record: found
- Abstract: found
- Article: not found
Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline.
- Record: found
- Abstract: found
- Article: not found